 Second International Fascia Research Congress Second International Fascia Research Congress
Second International Fascia Research Congress Second International Fascia Research CongressThomas W. Findley, MD, PhD
Center for Healthcare Knowledge, VA Medical Center, East Orange, NJ, USA
Findings from papers published by key speakers at the 2007 Fascia Research Congress are presented in preparation for the second congress, October 2009, in Amsterdam.
The role of fascia is demonstrated in new scientific findings in
- mechanotransduction between the cytoskeletal structure and the extracellular matrix, and its implications for health and disease.
- the presence of contractile cells (myofibroblasts) within the fascial fabric. Clinicians are interested in their role in creating contractile tonus in the fascial fabric—how myofibroblasts form, how they are activated, and their influence on passive muscle tonus.
- the biomechanical properties of fascial tissues: creep, relaxation, hysteresis, effect of sustained spinal flexion on lumbar tissues, strain-induced hydration changes, myofascial manipulation, and fascial viscoelastic deformation. These properties underlie the response of these tissues to therapy.
- how fascia is innervated, and how proprioception and pain are created, detected, and modulated by the spinal cord and the rest of the nervous system.
- forms of mechanical signaling within the fascial matrix, such as the tugging in the collagen matrix created by twisting acupuncture needles.
- new techniques for measurement of fascial motion in living tissue.
KEYWORDS: Fascia, musculoskeletal manipulation, research, congresses
The purpose of this editorial is to provide the reader with relevant information in preparation for the Second International Fascia Research Congress to be held in Amsterdam, October 27–30, 2009 (http://www.fasciacongress.org). As at the first congress, we expect attendance both by professionals involved in the therapeutic manipulation of this body-wide structural fabric and by scientists whose research interests are the body’s connective tissue matrix.
For the second congress, each scientific talk will conclude with clinical applications, and discussion time for clinicians to ask questions is planned. The main scientific presentations have been expanded to four days to allow more time to absorb and process information and to stimulate more discussion. One day of post-congress workshops specifically geared toward practitioners has been added on October 31.
Background papers from the first congress were compiled with the submitted abstracts and made available at the congress. This editorial reviews the papers from the key speakers at the main 2007 congress that are in the 2007 proceedings (available for ordering online at http://www.fasciacongress.org/2007/proceedings-book-order.htm ).(1) A glossary of scientific terms in the papers is now available.(2) These papers were selected to provide a wide overview of scientific issues in fascia research. Readers of the International Journal of Therapeutic Massage and Bodywork are encouraged to use them in preparation for the 2009 congress and to come with questions. Questions may also be submitted to me in advance at info@fasciacongress.org. Please indicate whether the question deals with research, education, or practice, and from which key speaker and congress year (2007 or 2009) it comes.
Fascia is the soft-tissue component of the connective tissue system that permeates the human body, forming a continuous, whole-body, three-dimensional matrix of structural support. It interpenetrates and surrounds all organs, muscles, bones, and nerve fibers, creating a unique environment for body systems functioning. The scope of our definition and interest in fascia extends to all fibrous connective tissues, including aponeuroses, ligaments, tendons, retinacula, joint capsules, organ and vessel tunics, the epineuria, the meninges, the periostea, and all the endomysial and intermuscular fibers of the myofasciae. There is a substantial body of research on connective tissue generally focused on specialized genetic and molecular aspects of extracellular matrix. However, the study of fascia and its function as an organ of support has been largely neglected and overlooked for several decades, with the number of publications rising each year, particularly recently (Fig. 1).
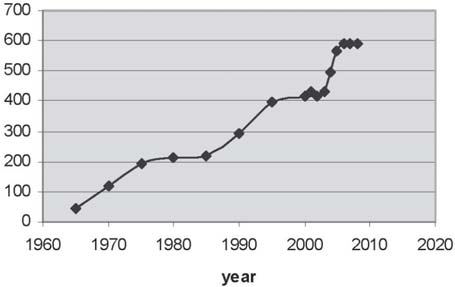
FIG. 1. Number of Medline-indexed publications each year with the term “fascia” in the title, abstract, or subject heading.
Hypotheses that accord myofascia a central role in the mechanisms of therapies have been advanced for some time in the fields of acupuncture, massage, structural integration, chiropractic, and osteopathy. Practitioners in these disciplines, especially those that do not have the longevity of osteopathy or chiropractic, are generally unaware of the scientific basis for evaluating such hypotheses. Many practitioners are unaware of the sophistication of current laboratory research equipment and methods. Laboratory researchers, in turn, may be unaware of the clinical phenomena that suggest avenues of exploration.
Among the various kinds of tissues that are involved in musculoskeletal dynamics, fascia has received comparatively little scientific attention. Fascia, or dense fibrous connective tissue, nevertheless potentially plays a major and still poorly understood role in joint stability, in general movement coordination, and in back pain and many other pathologies. In anatomic displays, the fascia is usually removed so that the viewer can see the organs, nerves, and vessels, but this approach fails to appreciate the fascia that connects—and separates— these structures.
In particular, there is increasing interest in certain therapeutic communities concerning the role that fascia plays in musculoskeletal strain disorders such as low-back instability and postural strain patterns of all types, fibromyalgia, pelvic pain, respiratory dysfunction, and chronic stress injures, and in wound healing, trauma recovery, and repair. The role of fascia is demonstrated in new scientific findings in the following categories:
For the musculoskeletal system, Chen and Ingber(3) describe design principles that result in special improvements in performance. They first explain engineering principles of tension and compression, with emphasis on effects of architecture and pre-stress. Pre-stressing in biologic systems serves to obtain stability with minimum mass, providing rapid mechanical responsiveness to added stress and reducing loads on individual structures, thus reducing structural fatigue. A hierarchical organization of a few types of material in the musculoskeletal system allows for a broad spectrum of mechanical properties exhibited by bones, muscles, cartilage ligaments, and tendons (and other forms of fascia). The remodeling of bone in response to local mechanical stress, known as Wolff’s Law, results in deposition of bone in specific patterns that correspond to engineering lines of tension and compression. This molecular organization results in increased strength for less mass in the bony system.
The design principles carry through to the molecular level in other biologic tissues, including cartilage, tendons, and ligaments. In soft tissues composed primarily of collagen and elastin, the pre-stress is generated from active contraction of the myofibroblasts. Mechanical engineering at the cellular level begins with the observation that all living cells are contractile: In muscle cells, the contractile system is highly organized, and in other cells, the contractile elements are organized into a loose network. Cells have a structural framework that allows forces to be transmitted within the cell. The cytoplasm itself can locally alter its stiffness using changes in cytoskeletal polymerization. Living cells react to a mechanical stimulus on the cell surface by immediate changes in the cytoplasm and nucleus.
The basic design principles of the musculoskeletal system result in maximal use of tensile materials from the molecular to the whole-body scale. How the various elements are connected in a three-dimensional network is more important than the material properties of the individual components. Stability is achieved through pre-stress and geometric organization such as triangulation. Hierarchical organization of components structured on smaller and smaller scales results in overall structural efficiency. Finally, dynamic remodeling results in an ability to modify stiffness and flexibility in response to loading patterns experienced over time. The design principles in living systems can be described by the architectural system known as “tensegrity.” (“The word “tensegrity” is an invention: a contraction of “tensional integrity.” Tensegrity describes a structural-relationship principle in which structural shape is guaranteed by the finitely closed, comprehensively continuous, tensional behaviors of the system and not by the discontinuous and exclusively local compressional member behaviors. Tensegrity provides the ability to yield increasingly without ultimately breaking or coming asunder.”(4))
In this system, isolated compression elements are connected by continuous structure providing tension. In contrast, most fabricated structures rely on continuous stacks of bricks or similar compression objects. Even when pre-stress is incorporated, as in pre-stressed concrete, the stiffness in such fabricated objects remains constant regardless of the imposed stresses. In contrast, stiffness increases and stress loads are increased in living tissues and also in fabricated three-dimensional tensegrity structures. The tensegrity model suggests ways in which living tissues can sense and respond to mechanical stresses.
Langevin and Sherman(5) suggest a model for low-back pain that incorporates connective tissue plasticity with pain psychology, postural control, and neuroplasticity. They start by describing what is known about tissue structure abnormalities, psychological factors, changes in movement patterns, and increased peripheral pain sensitivity and brain cortical activation patterns in people with low-back pain. They suggest that connective tissue remodeling in people with chronic low-back pain may result from either increased stress (“overuse injury”) or consistent absence of stress leading to atrophy and fibrosis. The loose connective tissues surrounding and within the muscle fibers play important roles in the response of muscle tissue to mechanical stress and in the sensory input from that tissue.
The authors propose that connective tissue fibrosis occurs in the low back because of decreased activity, muscle spasm co-contraction or microtrauma, and neurally mediated inflammation. This model can be used to evaluate interventions that involve application of external forces (for example, massage, manipulation, and acupuncture), movement education such as tai chi and yoga, and general increase in activity level and conditioning. They rightly point out that “the development, testing and implementation of effective treatment strategies are highly dependent on understanding the pathophysiological mechanisms of the condition being treated.”
Grinnell(6) describes the ability of fibroblasts to reorganize collagen matrix in cell culture to a dense mass one tenth the original size. These mechanical forces are large enough to cause scarring and deformation in many body organs after injury. Applying a mechanical load to the fibroblasts results in generation of actin stress fibers within the cells and development of those cells into myofibroblasts; absence of a mechanical load for as little as 24 hours causes the same cells to become quiescent through the extracellular signal–regulated kinase pathway. Microscopic examination of the collagen matrix shows a vast difference in structure and organization of the fibroblasts depending on whether tension on the cells was released immediately or after 4 hours during culture. Because the collagen matrix contracts to the same degree in both cases, little attention has been paid to the differences in structure and cellular mechanisms that may signal contraction in the two models. Grinnell emphasizes that “cells use different signaling mechanisms for contraction according to whether they are mechanically loaded or unloaded at the time when contraction is initiated.”
Myofibroblasts are connective tissue cells that contain dense stress-fiber bundles composed mostly of alpha smooth muscle actin. First discovered by a group working under Gabbiano and Majono (see Montandon et al.(7)) in the early 1970s, the myofibroblasts have been shown to play a major role in wound healing and also to be involved in many other normal and pathologic contractile tissue processes. Most of these cells develop out of normal fibroblasts stimulated by the influence of mechanical tension and specific cytokines. A smooth muscle–like contractility enables these cells to maintain contractile force over long durations with little energetic cost. An increased presence of myofibroblasts is a driving factor behind chronic fascial contractures such as those in Morbus Dupuytren, plantar fibromatosis, excessive scar formation, and frozen shoulder. Recently, the presence of myofibroblasts (or myofibroblast-like contractile cells) has also been demonstrated for normal dense connective tissues such as joint ligaments, menisci, tendons, organ capsules, and others.
Gabianni’s review of myofibroblasts(8) emphasizes the heterogeneity of this cell type and proposes four different phenotypes of this versatile cell. Many important advances in understanding this new cell type are covered by Hinz and Gabbiani,(9,10) particularly the transition from normal fibroblasts to myofibroblasts and the role of force transmission between this cell and the extracellular matrix via specially developed adhesion complexes at the cell membrane.
Huijing(11) reviews available literature on myotendinous and myofascial force transmission in general. He suggests that muscles may be viewed as fiber-reinforced composite materials, and that cellular and extracellular space must both be considered. Muscle force transmission passes not only sarcomere to sarcomere through the tendon to the bony skeleton, but also sarcomere to myofascial complex and then to the muscle tendon and to other structures. The Huijing paper forms the basis for understanding more recent studies on myofascial force transmission.
Solomonow(12) then examines the role of ligaments in musculoskeletal disorders such as work-related low-back pain. He emphasizes the important sensory function of these fascial structures and their viscoelastic properties of creep and relaxation in response to extensive loading. These basic properties account for mechanical disorders such as sprain and joint laxity.
Neuromusculoskeletal disorders result from changes in kinesthesis and proprioception, particularly in cumulative trauma disorders. Olson et al.(13) explore the “flexion–relaxation phenomenon” in which trunk flexion from the standing position results in a myoelectric silent period of the lumbar posterior muscles, which is commonly attributed to a taking over of spinal stabilization by the passive stretch resistance of posterior lumbar connective tissues. Interestingly, this phenomenon is radically altered when trunk flexion is performed from a supine body position rather than from the classically used standing position. It is concluded that lumbar kinematics or fixed sensory motor programs by themselves are not sufficient to explain the flexion– relaxation phenomenon. Certain bodyworkers are accustomed to observing clinical differences in muscle and fascial motion between supine and standing body positions, and the Olson paper begins to establish the scientific parameters of those observations.
Simons and Mense(14) review muscle tone as it relates to clinical muscle pain. Muscle tone depends on the physical properties of the soft tissues—viscoelastic properties of the muscular and associated tissues, and anatomic limitations in motion—and the degree of electrical activation of the contractile elements of the muscle, both voluntary and involuntary (muscle spasm). These authors measured viscoelastic tone (by resonant frequency of the muscle) and elastic stiffness (by slow movements). In both cases, electrical activity of the muscle may or may not be detected by electromyography, but this determination is critical to knowing just what is being measured. Clinical usage and measurement of muscle tone is covered, as are definitions of mechanical properties of muscle. Muscle is thixotropic—that is, when first moved, it resists motion, but after the initial motion, viscosity decreases by up to a factor of ten. Similarly, the authors cover clinical usage and measurement of contracture and muscle spasms and also severe clinical conditions such as tension headache, torticollis, and night cramps. The reader will gain insight into clinical practice, definition of terms, and measurement, which are essential to research in this area.
Khalsa(15) provides a review of the system used to perceive musculoskeletal pain. In this system, peripheral and central neurons can both adapt from milliseconds to weeks after noxious stimuli. Sensory stimuli are sent from muscles over nerves that conduct at a wide range of velocities, from under 2 m/s to more than 100 m/s. Half of the sensory innervation of muscles is in the slowest category. Muscle nociceptors vary in mechanical thresholds and can be sensitized by a number of local chemicals. The response at the cellular level to local mechanical trauma in a muscle is described in detail. Different mechanisms may be involved for compression and for stretch.
Nerves and nerve sheaths are themselves innervated by the nervi nervorum. An experimental study in rats by Sauer et al.(16) showed that stimulation of the nerve and nerve sheath releases neuropeptides involved in inflammation. This finding supports the hypothesis that the nervi nervorum surrounding nerve axons plays an important role in the pain response, both musculoskeletal and neuropathic.
Langevin et al.(17) used ultrasound to image and quantify dynamic changes in human connective tissue structure. These techniques can be used to compare connective tissue structure with histologic study of the same tissue and can show changes in structure after acupuncture needle rotation.
Hand surgeon Guimberteau(18) has used in vivo dissections of the wrists in humans and in cows to examine the structure of subcutaneous tissues that allows sliding of the tendons. He identified a “multimicrovascuolar collagen dynamic absorption system” that allows gliding at all levels below the skin surface. This gliding structure seems to be present in fascial tissues throughout the body.
Langevin(19) suggests that connective tissue may transmit electrical, cellular, and tissue remodeling signals throughout the body, each in response to mechanical forces, but on different time scales. Many tissues, including collagen, display immediate local electrical gradients in response to mechanical stress. Mechanical contacts between fibroblast cells are actively altered within minutes. Finally, tissue remodeling has been shown in tendons, ligaments, and joint capsules, and if this process is also present in loose connective tissue, it would provide a body-wide pattern for remodeling connective tissue based on movement and local tissue stress. Interactions among these three systems could provide both short-term and long-term responses.
Dr. Findley receives limited travel reimbursement and no salary support from the Fascia Research Congress. The conference itself received support through conference grant 1R13AT004146-01 from the National Center for Complementary and Alternative Medicine and the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The author declares that there are no conflicts of interest.
Published under the CreativeCommons Attribution NonCommercial-NoDerivs 3.0 License.
Corresponding author: Thomas Findley, University of Medicine and Dentistry of New Jersey, VA Medical Center, Mailstop 129, 385 Tremont Street, East Orange, NJ 07018 USA.
E-mail: tom.findley@gmail.com