 Directions and Dilemmas in Massage Therapy Research: A Workshop Report from the 2009 North American Research Conference on Complementary and Integrative Medicine Directions and Dilemmas in Massage Therapy Research: A Workshop Report from the 2009 North American Research Conference on Complementary and Integrative Medicine
Directions and Dilemmas in Massage Therapy Research: A Workshop Report from the 2009 North American Research Conference on Complementary and Integrative Medicine Directions and Dilemmas in Massage Therapy Research: A Workshop Report from the 2009 North American Research Conference on Complementary and Integrative MedicineChristopher A. Moyer, PhD1; Trish Dryden, RMT, MEd2; Stacey Shipwright, BA, RMT2
University of Wisconsin–Stout,1 Menomonie, WI, USA, and Centennial College,2 Toronto, ON, Canada
Background: Massage therapy (MT) is widely used and expanding rapidly, but systematic research on its mechanisms and effects has, in contrast with many other therapeutic fields, a short history.
Purpose: To take stock of the current state of MT research and to explore approaches, directions, and strategies with the potential to make the next two decades of MT research optimally productive.
Setting: The 2009 North American Research Conference on Complementary and Integrative Medicine held in Minneapolis, Minnesota.
Method: Using a modified Delphi method, the study authors led an interactive workshop that aimed to identify established MT research findings, needed MT research, weaknesses and limitations in currently available MT research, and directions to pursue in the next two decades of MT research.
Participants: The thirty-seven conference attendees—including MT researchers, educators, and practitioners, and other health care practitioners who already work interprofessionally with MT—actively participated in the workshop and ensured that a diversity of perspectives were represented.
Results: The MT field has made rapid and laudable progress in its short history, but at the same time this short history is probably the main reason for most of the current shortcomings in MT research. Drawing on a diversity of backgrounds, workshop participants identified many opportunities and strategies for future research.
Conclusion: Though lost time can never be recovered, the field’s late start in research should not be allowed to be a demoralizing handicap to progress. Modern scientific methods and technologies, applied to the range of directions and dilemmas highlighted in this report, can lead to impressive progress in the next twenty years of MT research.
KEYWORDS: Massage therapy, research, Delphi method, methodology, conference, mood, pain, anxiety, arthritis, lymphedema, cancer, stress, oxytocin, cortisol, effects, outcomes, operational definition, neuroimaging, profession, body awareness, dosage, medication uptake, therapeutic encounter, education, training, control group, professional standards, reductionism, whole systems, research literacy, protocols, integrative health, cost-effectiveness, longitudinal research
The practice of massage therapy (MT) is very old, but only in the last twenty years or so has scientific research on MT begun to accumulate. And although this growing body of research has certainly refined our understanding of MT and its effects, it is also true that it has serious shortcomings that hamper the field’s progress. To best ensure that the next twenty years of MT research will be of maximum value, the authors endeavored to take stock of established findings, to determine the new research that is most needed, and to identify consistent weaknesses that need to be addressed in this field. Logically, discussion of these topics should also lead to the identification of other issues that have the potential to inform the next two decades of MT research.
The 2009 North American Conference on Complementary and Integrative Medicine was a rare opportunity to assemble MT researchers, educators, and practitioners, and other health care practitioners who work interprofessionally with MT. The authors seized this opportunity by conducting an interactive, participatory workshop to identify needed directions and current dilemmas in MT research. This report presents the results of that workshop.
On Wednesday, May 13, 2009, the authors facilitated, at the 2009 North American Research Conference on Complementary and Integrative Medicine in Minneapolis, Minnesota, a ninety-minute workshop titled “Directions and Dilemmas in Massage Therapy Research.” The thirty-seven workshop participants (see Appendix) were asked to form subgroups of three to six people and to take approximately five minutes to introduce themselves to each other and to record their names, institutional affiliations, and email addresses on a provided handout. Next, the facilitators spent approximately fifteen minutes presenting a general overview of MT research progress covering the twenty-year period from 1988 to 2008. Finally, the remainder of the workshop was conducted by means of a modified Delphi method,(1) in which the subgroups generated responses to topics provided by the facilitators; subsequently, after each individual topic was addressed in the subgroups, the entire group reconvened to hear responses from the subgroups, to recognize consensus (or lack thereof) in the subgroup responses, and to engage in brief discussion.
The facilitators prepared five topics with corresponding instructions for the subgroups:During the workshop, a decision was made to skip topic number 3 (on methodological strengths) because of time limitations. The remaining topics were addressed in the order presented, with approximately an equal amount of time devoted to each.
Three techniques were used during the full-group portions of the workshop to ensure clear and accurate communication and recording of information. First, when subgroups were reporting their contributions to the larger group, an attempt was made to verbally reiterate the contributions, and the subgroups were provided with the opportunity to refine or restate their contributions in response to the reiterations. Second, an easel pad was used to visually organize and summarize the contributions of the subgroups. Third, after participants were properly informed, a shareware digital recording program (Audacity 1.2.6) running on a personal computer with an outboard boundary microphone was used to make an audio recording of the entire ninety-minute workshop.
Before the participatory portion of the workshop, the information in the subsections that follow was presented as an overview of the previous twenty years of MT research. This presentation helped to ensure that the diverse group of participants would begin the workshop with a common knowledge base. Approximately fifteen minutes total was devoted to covering the four topics that follow.
Quantity of MT Research
A rapid increase in MT research has occurred during the 20-year period from 1988 to 2008. Proof of this can be demonstrated by a year-to-year search in any of a number of scholarly or scientific databases such as PubMed, PsycInfo, or CINAHL. However, for the purpose of the workshop, the publicly accessible and wide-ranging Google Scholar database (
http://scholar.google.com
) was selected, allowing anyone with basic Internet access to replicate the procedure.
As shown in Fig. 1, the quantity of documents retrieved with the keyword “massage therapy” in the three most relevant Google Scholar subcategories increased dramatically during the selected time period. Note, however, that the raw numbers can be misleading; only a small portion of the retrieved documents represents original research, and only a portion of those will be of high quality. (For example, a 2004 metaanalysis identified only thirty-seven MT studies of sufficient quality for inclusion(2).) However, even with this in mind, the overall trend is still evident: the quantity of scholarly and scientific writing on MT increased rapidly from 1988 to 2008.
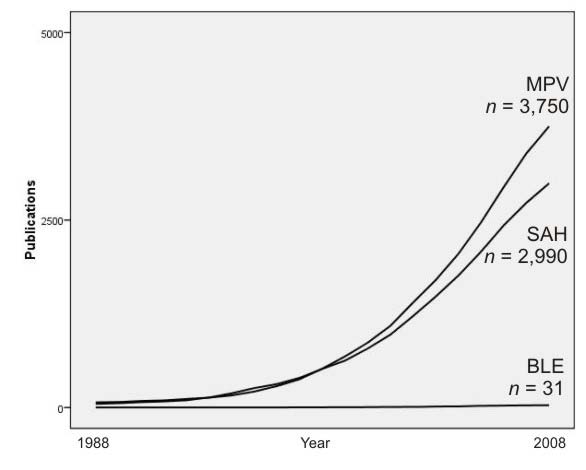
FIG. 1. Number of documents retrieved, in a year-by-year search using the keyword “massage therapy,” from three Google Scholar database categories. BLE = biology, life sciences, and environmental science; MPV = medicine, pharmacology, and veterinary science; SAH = social sciences, arts, and humanities.
At first glance, this progress appears remarkable. There are now several thousand MT documents, when just twenty years ago there were essentially none. But before the field can be certain that it is entitled to a self-congratulatory pat on the back for such amazing progress and impressive present-day totals, a comparison that puts those results into context would be useful. Is this pattern of results unique to MT, or would this general pattern be found for any number of related searches that might be conducted? Similarly, it might be questioned whether the remarkably low numbers in the earliest years are an accurate representation of the state of MT research during that time period, given that this result could just as easily be an artifact rooted in the idiosyncrasies and relative newness of the particular database being searched.
Many comparisons are possible (and we encourage interested readers to make them), but we believe that psychotherapy is a logical choice because of the many parallels that exist between it and MT. For instance, both forms of treatment(2)
As can be seen in Fig. 2, the same search procedures conducted with the keyword “psychotherapy” yield a very different result. There are so many more documents that a different scale for the vertical axis is necessary so that results can be displayed in the tens of thousands, instead of just thousands. Moreover, for these results, it makes sense to display linear regression lines rather than the raw data, a process that smoothes minor retrieval anomalies that can result when the search yield is large. Clearly, there has been much more scholarly writing and scientific research on psychotherapy than on massage therapy, such that the result of a comparison is humbling.
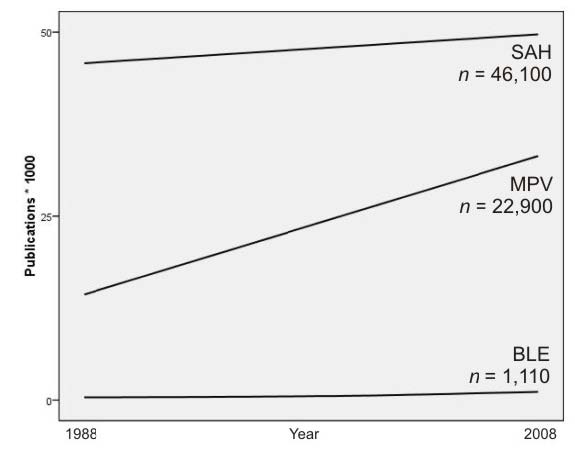
FIG. 2. Linear regression lines corresponding to documents retrieved, in a year-by-year search using the keyword “psychotherapy,” from three Google Scholar database categories. BLE = biology, life sciences, and environmental science; MPV = medicine, pharmacology, and veterinary science; SAH = social sciences, arts, and humanities.
In sum, it is undeniably true that MT research progressed dramatically over the twenty years in question. At the same time, though, it is also true that the field is probably far behind where it could be and that it has a long way to go. It is important for us to recognize that MT research is still in its infancy.
MT Research Reviews
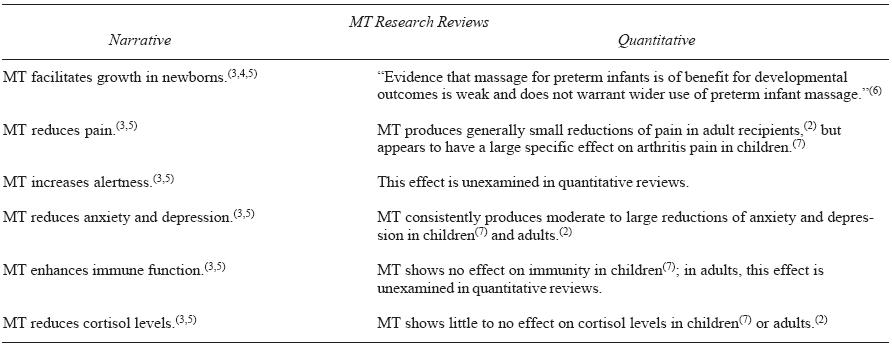
A number of MT research reviews were published during this period. A detailed account of them is beyond the scope of the current report, but it is worth noting that the results of narrative MT research reviews (in which review authors rely heavily on the written conclusions of the original studies) and those of quantitative MT research reviews (in which review authors measure treatment effects by applying statistical procedures to the actual data reported in the original studies) often diverge in their basic findings. Table 1 highlights some of the discrepancies.
TABLE 1. Comparison of Basic Conclusions Reached by Narrative and Quantitative Massage Therapy (MT) Research Reviews
Meetings to Determine Directions for MT Research
At least two important meetings have attempted to chart the direction for research on MT and related therapies. In 2002, the American Massage Therapy Foundation (now known as the Massage Therapy Foundation) reported the conclusions of its Massage Therapy Research Agenda Workgroup(8), which emphasized five main recommendations for the field. Specifically, it was recommended that the field
In general, these recommendations seem to have driven meaningful progress in MT research, including the establishment of several Massage Therapy Foundation initiatives such as their research grant program, separate student and practitioner case report contests, the International Journal of Therapeutic Massage and Bodywork (IJTMB), and the MT-specific research conference detailed later in the present report.
In 2005, the National Center for Complementary and Alternative Medicine (NCCAM) sponsored the Conference on the Biology of Manual Therapies(9) to bring together US and Canadian health experts and members of academic, patient advocacy, and professional organizations to assess current knowledge and to identify opportunities for further research in manual therapies such as MT and chiropractic and osteopathic manipulation. Numerous directions for research were organized under three main headings:
Apart from the intended influence of this fairly recent and more broadly-focused conference on NCCAM’s research agenda and funding priorities for manual therapies, its impact is difficult to assess. Notably, though, the broader focus of the conference may have been its most valuable element, given that it required attendees “to step out of our individual disciplines and look together at what we collectively know about the effects of manual therapeutic techniques.”(10)
MT-Specific Research Conferences
Although there have been scientific conferences concerned with the broader field of touch-based therapies (most notably, the outstanding International Symposiums on the Science of Touch in 2002 and 2004(11)), the first MT-specific research conference was not held until 2005 in Albuquerque, New Mexico. The Highlighting Massage Therapy in Complementary and Alternative Medicine Research conference(12) combined terrific networking opportunities with a healthy amount of quality research presentations and demonstrated that the interest and activity in MT research is sufficient to support a dedicated conference. The recent announcement of a second such conference to be held in 2010 in Seattle, Washington, is an exciting development.(13)
Research into MT progressed rapidly during the 1988–2008 period, and there is now sufficient interest and productivity to support the first conferences and journals dedicated to research in the field. At the same time, it must be acknowledged that, where research is concerned, the field is still in its earliest stages, and in a comparative sense, MT is significantly behind fields that have a dedicated research infrastructure. This perspective, presented to workshop participants, set the stage for the subsequent discussions.
Directed to “indicate MT effects, mechanisms, processes, or other details that are already relatively well understood as a result of research,” workshop subgroups chose the conclusions that follow as the most important ones to report to the full group. The order in which they were discussed in the workshop is preserved here.
However, the format and time limitations of the workshop did not allow for the provision of specific references; these were researched and added when the present report was written.Effect on Mood
The effect of MT on mood was nominated as an established effect. Note, however, that workshop time limitations did not allow for a detailed discussion of the fact that the effect of MT on negative mood does not attain statistical significance when quantitatively reviewed in adult(2) or child(7) populations.
Reduction of Musculoskeletal Pain, Including Low-Back Pain
Massage therapy is known to reduce some forms of musculoskeletal pain. It was noted that assessment of the effect of MT on pain more generally can be problematic, because averaging or otherwise combining the results of MT for different painful conditions may not be justifiable if it means that a robust effect on one condition may be washed out when combined with a lack of effect on another condition. For instance, one Cochrane review of MT for low-back pain indicates that this form of treatment “might be beneficial for patients with subacute and chronic non-specific low-back pain”(14). Another Cochrane review of MT for mechanical neck disorders concludes that “no recommendations for practice can be made at this time because the effectiveness of massage for neck pain remains uncertain.”(15) A very recent study of MT for chronic neck pain, which has not yet been incorporated into the continually-updated Cochrane reviews, finds that “therapeutic massage is safe and may have benefits for treating chronic neck pain, at least in the short term.”(16)
Reduction of Anxiety
The effect of MT on anxiety was noted as one of its most well-established effects.(2,7) Further, one of the subgroups echoed a point made in a recent IJTMB editorial, which noted that this effect may be especially important because it may be a main effect that is the foundation for a host of other, secondary effects associated with MT.(17)
Arthritis
The beneficial effects of MT for arthritis were nominated as established, and there is evidence to support this nomination. However, it is remarkable how little research is actually available on MT for arthritis, given the prevalence of that condition(18,19) and the promising results for MT in two studies. In a 1997 study of children with mild-to-moderate juvenile rheumatoid arthritis,(20) MT greatly outperformed relaxation therapy for reducing the pain associated with the condition. Similarly, a more recent study of adults with osteoarthritis of the knee(21) found that MT significantly outperformed a wait-list control condition for reducing pain and improving physical functioning.
Lymphedema
Reduction of lymphedema, the swelling of a limb resulting from a blockage of the lymphatic system, was offered as an established MT effect. A large-scale (n = 299) prospective study of multimodal treatment for lymphedema concluded that lymphatic MT, in combination with other treatments such as compression bandaging, remedial exercises, and skin care, was highly effective.(22) In addition, MT is endorsed by the Mayo Clinic as a treatment for lymphedema.(23)
Amelioration of the Effects of Cancer Treatment
A diagnosis of cancer, and the associated treatments, is stressful to patients.(24,25) Although not itself a treatment for cancer, MT can be effective in combating the stressful effects of the diagnosis and treatment. A number of studies(26–33) suggest that there may be specific effects of particular benefit to cancer patients, including reductions in anxiety, nausea, and pain, and improvements in appetite and sleep.
Stress Reduction
The ability of MT to reduce stress was nominated as an established effect. Taken at face value, this nomination seems obvious; but in scientific practice, the concept of “stress reduction” has been operationally defined in so many ways that saying precisely what “stress reduction” is may be difficult.(34) In a recent review, the stress-reducing effects of MT were examined by means of treatment-induced changes in physiological parameters such as cortisol level, heart rate, and blood pressure. Findings were mixed, and the researchers observed that the primary studies generally lack “the necessary scientific rigor to provide a definitive understanding of the effect massage therapy has on many physiological variables associated with stress.”(35) Based on currently available evidence, it may be pragmatic to consider MT to be a form of emotion-focused coping(36) that works by improving a recipient’s affective state,(17) which in turn reduces the perceived effect of negative stressors.
Increased Oxytocin
Oxytocin is a neuropeptide that plays a key role in mammalian social attachment and affiliation.(37) Under certain conditions, MT may lead to an increase of oxytocin consistent with feelings of well-being, with prosocial behavior, and with promotion of health. In a fascinating study that examined the interactions of physical contact and trust, Morhenn et al.(38) found that fifteen-minute doses of moderate-pressure MT increased oxytocin levels if they were followed by an intentional act of trust performed during an experimental procedure known as the “trust game.” Further, the MT recipients who participated in the trust game made larger altruistic sacrifices of money during the trust game than did individuals who played the trust game without first receiving MT. Increased oxytocin was not observed in a group of participants that received MT only, nor in a group that played the trust game without first receiving MT.
After briefly discussing these “well understood” effects, workshop participants raised a question: How, exactly, should “well understood” be defined? There is no simple answer, but the question is an important one for the field to consider.
The effect of MT on anxiety is probably the one best supported by scientific evidence, and that effect has been examined only in a few dozen high-quality studies. Some other effects nominated as “well understood” have been studied only a handful of times. The concept of “well understood” can probably be applied only in a relative way. For example, within the field, it would be accurate to say that the effect of MT on anxiety is better understood than its effect on arthritis, simply as a function of the number of studies that have examined each of those effects. And, although comparisons across fields are conceptually harder to make, it would almost certainly be accurate to say that MT is not as well understood as psychotherapy, which is also a conclusion based on the number of studies that have examined each of these forms of treatment. In either case, it should be clear that further research is needed, even on the “well understood” effects.
Next, the subgroups reconvened and worked together to “indicate MT effects, mechanisms, processes, or other details that are most in need of research.” The effects discussed in the subsections that follow are those considered important enough to report to the entire group. They are presented here in the same order as they were discussed in the workshop, with the exception of a topic that the authors moved to the “Conclusions” section for organizational purposes.
Multidimensional Studies
Workshop participants believed that individual MT studies have too often been limited to one “type” of outcome, where examples of such types might be self-report, behavior, or biochemistry, among others. Individual MT studies that assess multiple outcome types would be preferable in many, if not all, cases, because they would make greater use of the resources committed to a study and would permit examination of the degree to which different MT outcome types converge.
What Is MT?
As an umbrella term, MT can include all manner of theoretical assumptions, levels of training, specific strokes, variations in pressure, special techniques, and anatomic sites to which treatment is applied. Despite this inclusiveness—or, possibly, because of it— researchers often include only the most basic information on what constituted MT in a particular study. To improve matters, researchers can and should take care to indicate, in detail, what they mean when they report having examined “massage therapy.” This information would facilitate experimental replication and increase the potential of research to inform practice.
Neuroimaging Studies
Modern technology makes it possible to see what happens in the brain and the extended nervous system in response to treatment, and a few studies have examined the effect of MT on brain activity (for example, Diego et al. 2004(39)). Still, more studies that use the range of neuroimaging methods to examine the effects of MT are certainly needed, because an increased understanding of the effect of MT on central and peripheral nervous system activity is likely to be especially valuable.(40)
Studies That Define the Profession
Just as it can be hard to say precisely what MT is, it can be equally difficult to meaningfully define the field’s practitioners. Levels and types of training can vary widely between states, regions, territories, and countries; in some cases, health care practitioners who are not specifically or traditionally trained as massage therapists may still provide MT as part of health care delivery (for example, nurses, chiropractors, physical therapists, and so on). This situation raises a question: Who, exactly, is a massage therapist? Studies that examine the relationship between amount and type of training, the tasks and techniques that such training makes possible, and the outcomes that a practitioner is able to achieve could be valuable additions to MT research. Similarly, it is important for all MT research studies to provide detail on the background, training, and specialties of the massage therapists who provide treatment. This specificity has been absent in many study reports.
Body Awareness As a Mechanism of Action and As an Outcome
Some MT effects may result from the treatment’s potential to improve a recipient’s sense of their own body. This improvement could take several forms, such as enhanced proprioception, improved body image, or reduction of dissociation. In some cases, these outcomes may be desired in themselves. Although a few studies have examined these interesting possibilities,(41–43) more research is necessary.
Examinations of Dosage
An examination of dosage is fundamental to understanding a treatment, and relatively little is known about optimal dosing in MT. For a given condition, what constitutes an effective and efficient treatment dose? What constitutes an effective and efficient maintenance dose?
Effect of MT on Medication Uptake
It is possible that, for certain conditions, MT benefits patients by improving how, or triggering when, the body utilizes medications.(44) This interesting application of MT is certainly worth scientific investigation.
What Takes Place in the Therapist During MT?
We know some of what takes place in a recipient during MT, but we know hardly anything about what takes place in the therapist. Examination of intra-therapist processes that take place during treatment, including both physiological and psychological processes, could serve to improve MT training, to help identify optimal treatment and working conditions, and to promote career satisfaction, to name just a few interesting possibilities.
Studies of the Nature of the Therapeutic Encounter
Undoubtedly, effective MT depends on more than just the manual manipulation of soft tissue. Therapists and recipients are thinking, feeling people who communicate and form impressions of each other, and all of this interaction takes place within an environmental context that inevitably shapes the encounter. Research that examines the nature of these therapeutic encounters to identify factors in the therapist, recipient, environmental context, and ways that the foregoing can interact to produce desired outcomes has great potential to inform the field.
Education and Training Research
Training and education are critical to the success of a profession. What is the knowledge content that is essential to good practice? How much training is necessary to consistently yield competency? Which methods for teaching and training MT students work best? Does the amount or type of training that a MT student receives predict career satisfaction, success, or tenure? These and other questions pertaining to MT education and training are all worthy of study.
Workshop subgroups convened once more to “indicate ways in which MT research, as a field, has failed to use scientific methods, tools, and approaches to optimally increase our knowledge of MT.” Subsequently, the following seven topics, in the order reported here, were presented by the subgroups to the larger group.
Lack of Standards in the Profession
As noted earlier, the training, education, knowledge of research, and clinical experience of massage therapists varies widely, so much so that it can be difficult to precisely define what a “massage therapist” is. The resulting lack of commonly-held knowledge across the profession limits the contribution that massage therapists are able to make to MT research.
What Is a Good Comparison or Control in MT Research?
Most often, it is desirable for MT research studies to compare the effects of MT with another form of treatment (or, in some cases, to no treatment at all). This approach controls for confounds such as attention, expectation, spontaneous improvement, passage of time, and statistical regression, so that the most accurate determination can be made concerning the amount of improvement that is directly attributable to MT. But to what, exactly, should the control group be subjected?
In most medical research, the choice is straightforward. Control group participants should receive a placebo that is identical to the real treatment in all ways but one: the placebo does not deliver the active ingredient being examined in the study. Ideally, placebo-controlled studies must be double blind, which means that neither the study participants nor the researchers know who is receiving the active treatment and who is receiving the placebo until the results have been generated. This design feature ensures that both the active treatment group and the placebo control group will be equally affected by the previously mentioned confounds, such that any additional improvement observed in the active treatment group must be attributable to the active ingredient that only they have received.
It would be ideal if the logic of double-blind placebo-controlled studies could easily be extended to MT research, but in most cases, it cannot. The reason is not that any so-called alternative medicine treatments are somehow antithetical to scientific examination, as is sometimes claimed.(45) Rather, the reason is very simple: there is no way to blind the massage therapists participating in a research study. They obviously must know whether they are administering a real treatment, and this knowledge and the resulting expectations can always, even inadvertently, be communicated to the treatment recipient. Notably, the exact same problem arises in psychotherapy research.(46)
To what, then, should MT be compared? A related question that must also be asked is how does the eventual selection of a particular comparison or control condition affect the interpretation of a study’s results? There are no simple answers to these questions. Rather, it is incumbent upon MT researchers to make thoughtful choices and to clearly communicate the logic behind them. It is also necessary that many different comparisons be made, such that the idiosyncratic strengths and weaknesses of individual studies can complement each other and the results be considered together to best address the questions that MT research asks.
Restriction in the Range of Outcomes That Have Been Assessed
Some workshop participants felt that the field has inadequately assessed both the physiological outcomes of MT and the patient- or recipient-centered outcomes that motivate individuals to receive this form of treatment.
An Overemphasis on Reductionism at the Expense of Ecological Validity and the Whole System
As is evident from a recent exchange in the IJTMB,(47–49) the value of, need for, and even the proper definition of reductionism as it applies to MT research can be vociferously debated. Reductive methods in clinical research are sometimes criticized because they may remove a treatment from its context in a way that harms the treatment’s effectiveness, or because they may not allow for customization and individualization upon which a major portion of a treatment’s effectiveness may depend.(50) A solution is to design and conduct research that maximizes ecological validity, such that study details maintain or closely resemble the way a treatment is conducted in the real world.(51) Some complementary, alternative, and integrative medicine researchers emphasize ecological validity in whole-systems research.(52) Regardless of the terminology that the MT field may adopt, it is certainly true that standardized and laboratory-based MT research must be complemented with studies that more accurately reflect how this form of treatment is delivered in the real world. Further, if the results of these approaches to MT research do not converge, it is essential to conduct further research that can uncover the source of the discrepancies.
Lack of Research Literacy Among Massage Therapists
As was noted earlier, the field of MT lacks a research tradition and infrastructure. The result is that most massage therapists are not accustomed to reading, participating in, or benefitting from research. Increasing research literacy is likely to benefit the practice and profession of MT.
When Research Questions Are Driven by Methodology
A field’s progress can be limited by dependence on a narrow set of research methods. If there is familiarity or comfort only with, say, the randomized controlled trial, important questions that can be answered by a qualitative approach, survey method, case study, or naturalistic observation may never even be asked. Workshop participants noted that careful consideration of research questions should precede the selection of a research method, which is sound advice that all researchers need to be reminded of occasionally.
Confusion of Within-Group and Between-Groups Effects
Many between-groups MT studies (that is, studies that compare the effects of MT against another treatment or against no treatment) carelessly emphasize within-group effects (the before-and-after changes that take place in just the MT group) in their analyses and results.(53) This misleading practice could be problematic in any treatment field, because it fails to separate treatment effects from placebo effects and other confounds, which has the effect of distorting and obscuring the true effects of the treatment under examination. The problem is made worse when it occurs in a field such as MT, which lacks a strong research tradition, because most of the research consumers will not be in a position to critically evaluate methodologies and analytical strategies and must instead depend on the narrative description of the results provided by the researchers. The solution is, in essence, a simple one: MT researchers need to specify and conduct the correct analyses for their research design, and journal reviewers and editors must ensure that this criterion has been satisfied before agreeing to publish a study.
It was finally determined that time was insufficient for the subgroups to reconvene to discuss the last of the planned topics. Instead, the larger group was asked to give their thoughts in response to this question: “After considering what MT has, and has not, accomplished in the previous 20 years, what, as a field, is most important for us to consider as we go forward in the next 20 years?” The issues and topics that follow were raised. The repetition of a point that was already covered in detail in an earlier subsection has been omitted. These points have also been slightly reordered for better organization and emphasis in this section of the report.
The point was made that, because MT researchers are rarely practicing MT clinicians, they may be disconnected from some of the most important issues and questions that are arising from practice. As MT research moves forward, researchers should endeavor to stay in close contact with clinicians to build collaborative interprofessional research teams and to ask clinicians for their perspectives on needed research.
Several problems surrounding the area of MT research protocols must be addressed. One is that protocols are often poorly described in research studies. Future studies need to improve upon vague descriptions in the form of “15 minutes of Swedish massage was performed on the upper body.” Protocols need to be reported in sufficient detail, and with clearly-defined terminology, to permit precise replication and to aid in the eventual examination of the differential effectiveness of particular MT techniques, modalities, and dosages.
Progress can also be maximized by ensuring that research protocols reflect how MT is performed in practice. Addressing this important detail by means of close collaboration with working therapists helps to maximize the ecological validity of studies and increases the value of research to the field.
Additionally, there is also a need for greater standardization of MT protocols in MT research. At first, this assertion may seem to contradict the point just made—that MT research protocols must reflect practice in the real world. In actuality, these points are not mutually exclusive, and both are needed. Standardization of techniques, procedures, and guidelines for clinical decision-making, when accompanied by accurate and detailed description in research reports, permits meaningful comparisons that eventually lead to progress in clinical settings.
It is insufficient for researchers to specify a protocol and then to assume that the protocol unfolded in the study exactly as planned. High-quality MT research should also evaluate the clinical processes that emerge in the course of research and should report on the fidelity with which protocols were carried out. Logically, the hope is that research proceeds as planned and that fidelity to specified protocols is high, but it is always better to check. And, even when research does not proceed as planned, unexpected events and details, and instances in which the treatment diverges from that which was planned, have great potential to inform future research and practice.
Finally, the quality of MT research could probably benefit from agreement on a set of reporting standards. It was pointed out that, all too often, some important detail about a research study is omitted from the report. Adoption of formalized reporting standards for MT research, possibly based on the CONSORT guidelines,(54) could guide researchers and help to prevent such oversights.
It is terrific if an innovative, large-scale research design to address an important question can be devised, but the question will never be answered if funding to conduct the study cannot be obtained. And, in some cases, a strong and innovative proposal may fail to impress reviewers because they are unacquainted with how a proposal addresses some of the specific issues presented in this report, or because they dogmatically apply a rule of thumb that is frequently correct (for example, clinical research must have a placebo control group), but not applicable to a particular MT study proposal. This problem may be a difficult one to solve, but the field can do at least two things to address it. The first is to write clear research proposals that anticipate the blind spots some reviewers may have related to MT research. The second is that individuals with MT research expertise should, when opportunities arise, devote time to serving on research grant review boards and to educating colleagues in other clinical fields about some of the challenges present in MT research.
It was pointed out that there is value in expanding the research focus to examine how MT integrates with health and health care more broadly. When, where, and how is MT being used in health care settings and as a complement to other treatments, and what effect does MT have on the delivery and effects of other treatments? How should the contribution that MT makes to wellness and health maintenance be evaluated, in contrast with the more common practice of evaluating only the benefits that MT holds for certain conditions and symptoms? Does MT have a “professional identity crisis” that results from the fact it is performed alongside medical treatments in some settings, and as a personal service in other settings? Clearly, many interesting questions arise from a consideration of the broader role of MT in integrative health, and these need to be researched.
Results in the form of degrees added to range of motion, lowered scores on an anxiety measure, and statistically significant p values are fine, but in the end, money may be the best outcome metric of all, and it is one that the field has tended to ignore. Studies that assess the cost-effectiveness of MT have the potential to make a big impact and can lead to health insurance reimbursement when MT treatment is demonstrated to be economically viable.
All of the MT research of which we are aware has been limited to treatment periods of days or weeks. The result is that nothing scientific is known about the effects of MT applied across months or years. Longitudinal research that follows research participants for extended time periods is definitely needed and is likely to yield valuable and surprising results.
Within the field, agreement that MT benefits are not wholly attributable to the manual manipulation of the recipient’s body is probably universal. Manual manipulation is part of the way in which benefit is provided, of course, but surrounding that manipulation is a complex interplay of how the therapist and recipient think and feel about each other, their expectations of and attitudes toward MT, and their prior experiences (to name just a few factors that are probably important). Scientific examination of the complex interaction of multiple intangible variables is daunting, but in this case, it is also too important to ignore. Innovative ways to assess the therapeutic encounter must be developed if the scientific understanding of MT is to be improved.
The process of conducting the workshop, and of writing this report, identified many issues pertaining to MT research, and it may seem logical to assume that many are unique to the field. However, such uniqueness is almost certainly not the case. In fact, it is likely that each of these issues has already been encountered, and attempts made to address them, in related fields belonging to the wider world of applied and clinical research. Currently, MT research has many issues to address not because the field is unique, but because it is so young. As it matures, MT research will undoubtedly contribute innovations to the wider world of clinical research, but progress in the field itself will be maximized if proponents first acquaint themselves with how other clinical fields have addressed identical or parallel issues.
Massage therapy research has made considerable progress in the twenty-year period from 1988 to 2008, but that time period can also be seen as the infancy of systematic MT research. This places the field far behind many other health modalities, especially those with a research tradition and infrastructure. Although time lost can never be recovered, the field’s late start need not be a demoralizing handicap to progress. Indeed, it may even present certain opportunities and benefits. Consider how much more rapidly medical research could have progressed, and how many mistakes and dead ends avoided, if that research had begun with late twentieth- and early twenty-first-century methods and technologies. This situation is precisely the one in which MT, as a field, finds itself today. The technologies available in the Information Age ensure that proponents can communicate rapidly, collaborate efficiently, and maximally leverage the depth and breadth of modern scientific knowledge as they address the fundamental issues arising at this early stage of MT research. The progress that MT research makes in the next twenty years should be impressive.
The authors thank the individuals who participated in our workshop at the 2009 North American Research Conference on Complementary and Integrative Medicine. We also thank Glenn M. Hymel and Karen T. Boulanger for helpful feedback in response to a draft of this report.
The authors declare that there are no conflicts of interest.
Published under the CreativeCommons Attribution NonCommercial-NoDerivs 3.0 License .
Corresponding author: Christopher A. Moyer, Department of Psychology, University of Wisconsin–Stout, Menomonie, Wisconsin 54751 USA.
E-mail: christopher.a.moyer@gmail.com
| Participants | Affiliations |
| Lois Bogenschultz | Cincinnati Children’s Hospital Medical Center |
| Karen Boulanger | Massage Therapy Foundation and University of Iowa |
| MK Brennan | American Massage Therapy Association |
| Marissa Brooks | Massage Therapy Foundation |
| Dongyuan Cao | Palmer College of Chiropractic |
| Dan Cherkin | Group Health Center for Health Studies |
| Lisa Corbin | University of Colorado Denver |
| Susanne Cutshall | Mayo Clinic |
| Elaine Danelesko | Mount Royal College |
| Bernadette Della Bitta Nicholson | Commission on Massage Therapy Accreditation |
| Kinga Dziembowski | |
| Kathleen Farah | Children’s Clinic of Minnesota and Red Cedar Medical Center |
| Maura Fitzgerald | Children’s Hospital of Minnesota |
| Michael Hamm | Cortiva Institute-Seattle |
| Nancy Jallo | Virginia Commonwealth University |
| Anna C. Jensen | Northwestern Health Sciences University |
| Ania Kania | IN-CAM and University of Calgary |
| Hollis King | A.T. Still University School of Osteopathic Medicine |
| Romy Lauche | |
| Wolf Mehling | University of California–San Francisco |
| Martha Menard | University of Virginia School of Medicine |
| Jeremy E. Miller | Abbott Northwestern Hospital, Penny George Institute for Health and Healing |
| Adam Perlman | University of Medicine and Dentistry of New Jersey |
| Joel Pickar | Palmer College of Chiropractic |
| Katherine Pohlman | Palmer College of Chiropractic |
| Antony Porcino | University of British Columbia and University of Calgary |
| Cynthia Price | University of Washington–Seattle |
| William Reed | Palmer College of Chiropractic |
| Beatrix Roemheld-Hamm | University of Medicine and Dentistry of New Jersey |
| Jo Smith | Southern Institute of Technology |
| Kiyoshi Suzuki | MOA Health Science Foundation |
| Ann Gill Taylor | University of Virginia |
| Lesley Teitelbaum | Crouse Irving Hospital |
| Barb Thomley | Mayo Clinic |
| Diana Thompson | Massage Therapy Foundation |
| John Toews | University of Calgary |
| Ruth Werner | Massage Therapy Foundation |
INTERNATIONAL JOURNAL OF THERAPEUTIC MASSAGE AND BODYWORK—VOLUME 2, NUMBER 2, JUNE 2009