 Understanding the Process of Fascial Unwinding Understanding the Process of Fascial Unwinding
Understanding the Process of Fascial Unwinding Understanding the Process of Fascial Unwinding
Budiman Minasny, PhD
Australian Centre for Precision Agriculture, The University of Sydney, New South Wales, Australia
Background: Fascial or myofascial unwinding is a process in which a client undergoes a spontaneous reaction in response to the therapist’s touch. It can be induced by using specific techniques that encourage a client’s body to move into areas of ease. Unwinding is a popular technique in massage therapy, but its mechanism is not well understood. In the absence of a scientific explanation or hypothesis of the mechanism of action, it can be interpreted as “mystical.”
Purpose: This paper proposes a model that builds on the neurobiologic, ideomotor action, and consciousness theories to explain the process and mechanism of fascial unwinding.
Hypothetical Model: During fascial unwinding, the therapist stimulates mechanoreceptors in the fascia by applying gentle touch and stretching. Touch and stretching induce relaxation and activate the parasympathetic nervous system. They also activate the central nervous system, which is involved in the modulation of muscle tone as well as movement. As a result, the central nervous system is aroused and thereby responds by encouraging muscles to find an easier, or more relaxed, position and by introducing the ideomotor action. Although the ideomotor action is generated via normal voluntary motor control systems, it is altered and experienced as an involuntary response.
Conclusions: Fascial unwinding occurs when a physically induced suggestion by a therapist prompts ideomotor action that the client experiences as involuntary. This action is guided by the central nervous system, which produces continuous action until a state of ease is reached. Consequently, fascial unwinding can be thought of as a neurobiologic process employing the self-regulation dynamic system theory.
KEYWORDS: Fascia, palpation, massage, myofascial release, indirect techniques, musculoskeletal manipulations, mind–body relations, imagery
Fascial or myofascial unwinding is a process in which a client undergoes a spontaneous reaction in response to the therapist’s touch. Fascial unwinding can be used to “release” fascial restriction by encouraging the body or parts of the body to move to areas of ease. Mosby’s Dictionary of Complementary and Alternative Medicine defines fascial unwinding as a manual technique in which the therapist passively moves some part of the client’s body, with constant feedback as to the sensations of motion being given by the client.(1) Furthermore, the Glossary of Osteopathic Terminology(2) states that fascial unwinding is “a manual technique involving constant feedback to the osteopathic practitioner who is passively moving a portion of the patient’s body in response to the sensation of movement. Its forces are localized using the sensations of ease and bind over wider regions.” From these two definitions, we can therefore infer that fascial unwinding is a type of indirect myofascial release (MFR) technique.a
Therapists use an induction process to initiate fascial unwinding in a client. The client responds to the induction with spontaneous bending, rotating, and twisting of the upper or lower limbs or the whole body in either a rhythmic or a chaotic pattern. This response can be thought of as a spontaneous expression of movement. The phenomenon of unwinding, in which parts of the body move spontaneously and involuntarily, can appear mystical, and yet its therapeutic effects are known both anecdotally and clinically. These effects, however, are not well reported.
During treatment, the therapist acts as a catalyst or facilitator by placing the client’s body in certain configurations that allow it to unwind and release. The release is set in motion with the therapist’s touch, but the client soon takes control. Motion is usually induced in the body by lifting and holding certain body parts to remove the influence of gravity and to overcome the reactive proprioceptive postural tone—a technique often used when working with the limbs. According to Kern,(3) when the effect of gravity is removed, any strain patterns held in the tissues become more easily clarified. In an alternative method, the therapist adds compression to the joints in the area or holds a part of the body in a relaxed position. The unwinding process can be carried out either on the body as a whole or on specific body parts such as arms, legs, the neck, and even the jaw. For example, in arm and shoulder unwinding, the client lies supine while the therapist lifts an arm. The arm is then supported under the therapist’s elbow and wrist, and a light compression toward the shoulder joint can be added. After a while, the therapist will sense movements around the shoulder joint. The therapist then follows any hint of movement without directing or forcing it.
Although many research papers relating to fascia currently hypothesize about how MFR works,(4–6) unwinding is still a grey area: the mechanism is not well known. The most accepted explanation for unwinding is that tissues can hold memories that are independent of the nervous system,(7) but there are no scientific research studies to back that claim. Although scientific evidence shows that fascia can contract and relax,(8) an ability to “unwind” has not been shown. Ward(9) suggested that the seemingly random movements that characterize unwinding reflect a variety of interacting electromechanical events affecting central, peripheral, autonomic, and even physiologic functions. He added that “amid much speculation, satisfactory scientific descriptions for the events are lacking.”
In an endeavor to understand the process of unwinding, a literature review was conducted. A hypothesis that aims to explain the mechanism of the process was subsequently developed.
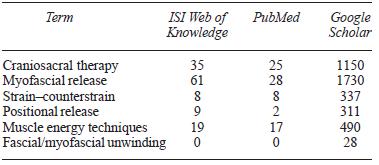
Searches using the terms “fascial unwinding” or “myofascial unwinding” were carried out in mainstream research databases: PubMed and ISI Web of Knowledge (Table 1). Although other related bodywork modalities were found, no result was obtained for unwinding. Google Scholar, a search engine that looks for scholarly literature across many disciplines and sources, including theses, books, abstracts, and magazine articles, identified only 28 articles.
TABLE 1. Articles for Various Manual Therapy Techniques in
PubMed, ISI Web of Knowledge, and Google Scholar as at February
Articles, manual therapy books, and scientific papers were reviewed and synthesized to find a possible explanation for the unwinding process. Based on that synthesis, I propose a hypothetical model to describe how and why unwinding occurs.
Ward(9) stated that the osteopathic origins of unwinding are unclear; however, the procedures have been described for decades by many osteopathic practitioners. Most indirect manipulative techniques such as unwinding are based on a common concept that the role of the practitioner is to encourage the inherent corrective activity or homeostatic physiologic mechanisms. In some references,(3,10) Dr. Viola M. Frymann, an osteopathic physician, is credited with developing the technique and coining the term “unwinding.” The physical unwinding component of somatoemotional releaseb is based on Dr. Frymann’s work.(10) Sills(11) preferred the term “macro-motions” to describe the process in which a client’s body expresses large motions. He avoided the term “unwinding” because of its connotations with “release.”
Although unwinding originated in osteopathic schools,(9) it is now also widely offered in classes that teach cranial or craniosacral therapy(12) and MFR.(13,14) By attending these classes, massage therapists obtain training in fascial unwinding techniques that they can apply in the context of their massage treatments.
The discussion herein is limited to the phenomenon of physical unwinding, which aims to release musculoskeletal pain and to allow greater range of motion. In some cases, emotional release can also occur or be induced during the unwinding process, but this secondary effect is not the subject of this paper. Although specific techniques can be used to initiate the unwinding process, unwinding itself can be viewed as a process that may occur when those techniques, or others, are applied to the body. Additionally, the unwinding process can occur around any articulation or group of articulations: for example, between the head and the neck, between regions or segments of the vertebral column, or between a limb and the torso. The agencies for motion are muscles, ligaments, and fasciae.(15)
Generally, unwinding is explained in bodywork literature as being based on the simple principle of the body’s ability for self-correction from mechanical disturbances.(13,15) That is, unwinding occurs because tissues hold memories of trauma and the unwinding process allows the body to adjust to a new position of ease. Sills(11) stated that the motions often signal the letting go of frozen stress responses and unresolved trauma.
In contrast to the tissue memory theory, ideomotor movement was suggested by Dorko(16) as a possible explanation of fascial unwinding. Ideomotor actions are unconscious, involuntary movements that are performed by a person and that may be caused by prior expectations, suggestions, or preconceptions. Ideomotor action has two important characteristics(17): first, the person is not aware of causing the movements, and therefore the movements are ascribed to an external force or power; and second, the movement feels unnatural, and thus the external forces perceived are usually regarded as being mystical or paranormal in nature. However, because these movements cause tangible effects, they can be repeated. Automatic writing, dowsing, and using Ouija boards to make contact with those in the spirit world have been attributed to the effects of this phenomenon. According to Dorko,(16) activities in which movement is thought to be caused by forces that transcend our senses or that are described as metaphysical in nature can be suspected to begin with movement that is not consciously planned.
In this paper, I propose a model based on scientific literature to explain the process and mechanism of fascial unwinding (Fig. 1). The model is based on the theories of ideomotor action by Carpenter(18) and Dorko,(16) fascia neurobiologic theory by Schleip,(4,5) and the psychology of consciousness by Halligan and Oakley.(19)
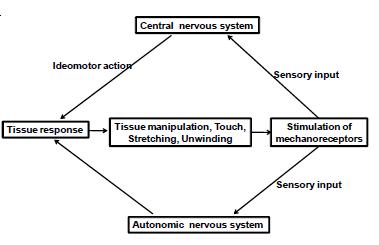
FIGURE 1. A hypothetical model for fascial unwinding (based on Schleip(5)).
A set of conditions are required to initiate or facilitate the unwinding process. The therapist’s sensitivity and fine palpation skills form the most important part of these conditions, but it is also imperative that the client be able to relax and “let go” of his or her body.
In the first stage—the initiation or induction phase— the therapist working on a client will introduce touch or stretching onto the tissue. Touch is the entrance requirement for the process of unwinding. Touch stimulates the fascia’s mechanoreceptors and, in turn, arouses a parasympathetic nervous system response.(5) As a result of this latter response, the client is in a state of deep relaxation and calm, sometimes followed with rapid eye movement, twitching, or deep breathing—a state that can be observed clinically.(20,21) In this state, the conscious mind is relaxed and off guard. Stimulation of mechanoreceptors also influences the central nervous system. The central nervous system responds to this proprioceptive input by allowing the muscles to perform actions that decrease tone or that create movement in a joint or limb, making it move into an area of ease. At this point, ideomotor reflexes occur. Ideomotor action pertains to involuntary muscle movement, which can manifest in various ways and is directed at the central nervous system.(22)
These reflexes occur unconsciously, indicating dissociation between voluntary action and conscious experience.(23) In clinical situations, the client is unaware of the unconscious movement and thinks that it is generated by the therapist. This unconscious movement or stretching sensation stimulates a response in the tissue, providing a feedback to the central nervous system as outlined in the theory of ideomotor action.(24) The process is repeated until the client is relaxed or has reached a “still point” or state of ease.
This general hypothesis is based on clinical observations and is backed up by scientific literature. However, it should be noted that not everyone will respond to the unwinding process and not everyone will go through the same process in the same way.
The three theories discussed next give rationalizations for the hypothesized model.
Neurobiologic Fascia Theory
Schleip(4,5) presents a comprehensive review of the neurobiology of fascia and provides a theory on how MFR works. In this theory, fascia and the autonomic nervous system are intimately connected. Fascia is densely innervated by mechanoreceptors that are responsive to manual pressure. Pressure from myofascial manipulation involves the stimulation of intrafascial mechanoreceptors whose signals are then processed by the central nervous system and autonomic nervous system. The response of the central nervous system changes the tonus of some related striated muscle fibers. The autonomic nervous system response includes an altered global muscle tonus, a change in local vasodilatation and tissue viscosity, and a lowered tonus of intrafascial smooth muscle cells.
The indirect stimulation of the autonomic nervous system (that is, the parasympathetic nervous system), which results in global muscle relaxation and a more peaceful state of mind, represents the heart of the changes that are so vital to many manual therapies. Gentler types of myofascial stretching and cranial techniques have also long been acknowledged to affect the parasympathetic nervous system.(25) Bertolucci(20) observed that, when a client is being treated with a muscle repositioning technique, the client begins to show involuntary motor reactions—reactions that include the involuntary action of related muscles and rapid eye movements. Several studies have evaluated the physiologic changes in the autonomic nervous system that occur as a result of craniosacral and MFR interventions,(21,26) clinically-known techniques that can trigger the unwinding process.
Recent studies have used heart rate variability, respiratory rate, skin conductance, and skin temperature as measures of physiologic change. Zullow and Reisman(26) indicated an increase in parasympathetic activity resulting from the compression of the fourth intracranial ventricle (CV4) maneuver and sacral holds, as measured by heart rate variability. Using heart rate variability measurement, Henley et al.(25) demonstrated that cervical MFR shifts sympathovagal balance from the sympathetic to the parasympathetic nervous system.
Fernandez-Perez et al.(21) examined the effect on physiologic changes of introducing three myofascial induction or craniosacral techniques. Anxiety levels significantly declined after the application of the three myofascial techniques. Heart rate and systolic blood pressure were altered during the course of the techniques, and the effects were observed for up to 20 minutes after the intervention. Boyd(27) showed that a combination of touch and CV4 technique is responsible for a decrease in brain wave activity—primarily in the frequency ranges associated with active nervous system function.
However, Milnes and Moran(28) demonstrated that the application of the CV4 technique in asymptomatic individuals had minimal physiologic effect in a range of autonomic response variables (heart rate variability, respiration rate, galvanic skin resistance, and skin temperature). Nevertheless, on examination of heart rate variability, those authors found that 3 of 10 subjects may have responded in a manner consistent with an increase in parasympathetic activity during the treatment phase, leading them to hypothesize that there may be both “responders” and “non-responders” to treatment.
Unwinding as an Ideomotor Action
Dorko(16) was the first to suggest that fascial unwinding can be simply explained as an ideomotor movement. McCarthy et al.(29) were the first to document unwinding as an ideomotor-based manual therapy in the treatment of a patient with chronic neck pain. Their research showed that a reduction in pain intensity and perceived disability can be achieved with the introduction of ideomotor treatment.
Ideomotor action or ideomotion is the “influence of suggestion in modifying and directing muscular movement independently of volition”—a definition given by psychologist and physiologist William Carpenter in 1852.(18) Carpenter used ideomotor action as an explanation for various phenomena that were being credited to new physical forces, spiritual intervention, or other supernatural causes.(30,31) Later, in 1890, William James(32) proposed a broader meaning: that ideomotor activity is the basic process underlying all volitional behavior. Ideomotor action also pertains to body movements that can arise in observers watching other people perform certain actions.(33) In other words, muscles can be involuntarily activated by thoughts. Moreover, involuntary muscle movement can manifest in various ways. For example, asking a subject to think of an activity can be enough to set the muscles required for that activity into action.(30)
In the mid-1800s, Carpenter(22) characterized ideomotor action as the third law of reflex. At that time, reflex movements were partitioned into two types: excito-motor (such as breathing and swallowing) and sensory-motor (such as surprise reactions to a loud noise). Carpenter imagined the processing of stimuli and the generation of action as a bottom-up path of information processing (Fig. 2). During the normal course of processing, external impressions evoke sensations, ideas, emotions, and intellectual processes that determine the “will.” Once this happens, the will initiates the actions to be executed.
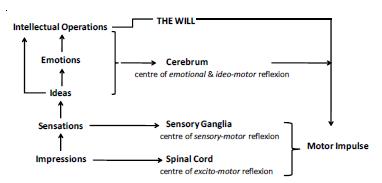
FIGURE 2. Processing of external information based on Carpenter’s model (Carpenter, 1860(22)).
Carpenter suggested that, should the processing path be interrupted at any point, a reflex action occurs.(34) His path of information processing comprises three levels. On the lower levels of the path are the excitomotor reflexes, which are controlled by the spinal cord. On the next processing level, sensory-motor reflexes set in, controlled by the sensory ganglia. And finally, on the highest level, the “ideo-motor” reflexes occur when the will, as the highest controller, is turned off in some way. When the ideomotor reflexes occur, ideas and emotions gain direct access to action execution through these reflexes (Fig. 2).(22)
A more contemporary study used functional magnetic resonance imaging of the brain to investigate the neural basis of ideomotor action.(35) According to contemporary ideomotor theory,(36) the typical reason for performing an action is to produce an effect in the environment. To perform an intentional action, the consequences or effects of a particular movement must be known. The ideomotor principle is based on two conditions(24): First, movements and their ensuing effects are required to become associated, so that prediction of an effect for any given movement is possible. Second, this association is bidirectional, so that anticipation of the required movement directly triggers the actions that have been learned to produce those effects.(36) This is the difference between sensorimotor and ideomotor learning. As an example, both types of learning may be present in playing the piano, but sensorimotor mapping would associate the finger movement to the sight of the musical note, whereas ideomotor learning would associate the finger movement to the hearing of the tone.(24) In unwinding, when it is initiated, the movement is guided by and associated with the stretching sensation, to find areas of ease of movement and freedom from pain. This result is contrary to that in stretching, in which the movement is guided by the therapist’s hand or instruction.
McCarthy et al.(29) suggested that the resolution of muscular pain depends on an appropriate motor response and that this response should proceed as the result of instinctive, in-built mechanisms. Ideomotor movements constitute the prevailing expression of instinctive movement mechanisms. McCarthy et al. therefore hypothesized that the corrective ideomotor movement expression may lead to improvements in pain intensity and disability in symptomatic clients whose instinctive responses have been suppressed.
Consciousness Model
In the field of psychology, the consciousness model is used to explain ideomotor action. Halligan and Oakley(19) suggested that all the thoughts, activities, ideas, feelings, attitudes, and beliefs traditionally considered to be the contents of consciousness are produced by unconscious processes—just like actions and perceptions. Only later, when they enter consciousness, does a person become aware of them as outputs.
In the model by Halligan and Oakley (Fig. 3), all the information-processing activities of the brain referred to as “unconscious” parts are designated Level 2. Within this level, there must be some kind of decision-making device—a central executive structure (CES). The CES identifies the most important task the brain is carrying out at any moment and selects the information that best describes the current state of the brain in relation to the chosen task. Only the selected information would be allowed to enter Level 1, to produce a conscious experience. During unwinding, Level 2 is processing information about the stimulation of mechanoreceptors and suggestion of movements. Because the autonomic nervous system is in a relaxed state, the CES does not select information for entry to Level 1, and the client remains unaware of it.
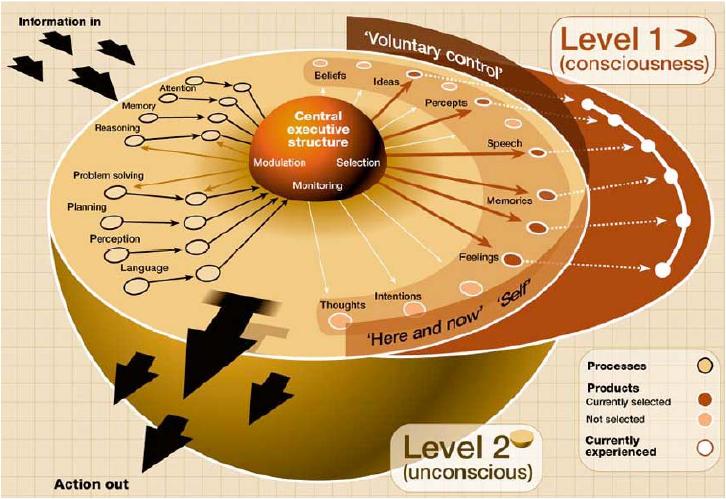
FIGURE 3. Mental process from thoughts to action (Halligan and Oakley(19)). © New Scientist, 2001. Used with permission.
In a hypnosis trial, Haggard et al.(23) showed that an ideomotor response produced by suggestion is generated by normal voluntary motor control systems, but is experienced as involuntary, resulting in a conscious experience close to that of a passive movement. Unwinding or ideomotor process thus represents dissociation between voluntary action and conscious experience. The trial also found that the participant typically estimates that the movement occurs earlier in time when it is a voluntary movement than when the same movement is made involuntarily. This finding suggests that the processes that precede voluntary movement include an unconscious planning stage that leads to an anticipatory awareness of the impending movement. Movements that are produced reflexively or by unwinding, on the other hand, lack the central planning stage, because the client is in a relaxed state. They are not accompanied by anticipatory awareness and are therefore experienced as occurring much closer to the time of the actual physical movement.
A model built upon the neurobiologic, ideomotor action, and consciousness theories is proposed to explain the mechanism of unwinding. Touch, stretching, and manual therapy can induce relaxation in the parasympathetic nervous system. They also activate the central nervous system, which is involved in the modulation of muscle tone as well as movement. This activation stimulates the response to stretching: muscles find areas and positions of ease, the client experiences less pain or is more relaxed, thereby introducing the ideomotor action. The ideomotor action is generated through normal voluntary motor control systems, but is altered and experienced as an involuntary reaction. The stretching sensation provides a feedback to the nervous system, which in turn will generate the movements again.
In bodywork literature, it is generally accepted that fascia or connective tissues can hold onto memories and trauma.(37,38) But the fact that a specific touch or body positioning can trigger a specific memory associated with the touch or positioning doesn’t mean that the particular memory is stored in those tissues or cells. Scientific evidence supports the effects of touch and positioning as potential “triggers” for a memory, but the memory is still “stored” within the central nervous system.(39,40) This occurrence is called state-dependent memory (coming from the observation that memory in one state of consciousness cannot be recalled until the person returns to the same state).(41)
This paper demonstrates that it is possible to develop a useful working model for the unwinding process based on the existing scientific literature. However, additional evidence and testable hypotheses are required to move this concept beyond the realm of what is often considered to be pseudo-science. To test the proposed hypotheses, investigations involving the two main processes—stimulation of the sympathetic nervous system(42) and analysis of ideomotor action—are required. These investigations will also require researchers to explore psychological processes and phenomena.(43)
Ideomotor action provides a sound explanation, but it also has another implication—that the perceived movement may be generated by the therapist while palpating. A therapist’s non-conscious perceptions— such as expectations, degree of empathy, and so on— can influence decision-making and leave open the possibility of the therapist falling into a self-fulfilling prophecy or “expectancy confirmation effects.”(30) As noted by Upledger,(7) “I can’t tell you how somatoemotional release works. I know that the intention of the therapist has a lot to do with it. Also the less guarded the patient is, the quicker it will work.”
The effect of myofascial manipulation has been studied from cellular to tissue to whole-body levels. Although fascia can contract and relax,(8) an ability to “unwind” has not been shown. Studies have demonstrated that it is impossible to generate immediate and permanent lengthening or “unwinding” of fascia by mechanical means. Creating such changes requires a large amount of force, with longer durations of stretching.(5) Stimulation of mechanoreceptors is the most likely trigger of a release that instigates the unwinding process.(4) Furthermore, application of force by manual therapists at the surface of the body over the tensor fascia lata and plantar fascia is not within the range required to mechanically stretch the fascia, although over softer tissues such as nasal fascia, the applied forces are sufficient.(44)
Finally, to relate unwinding to Schleip’s(5) bodywork model, the process can be viewed as an application of the neurobiologic concept using the self-regulation dynamic system theory. The therapist works as a facilitator—inducing the parasympathetic system; paying attention to the state of the autonomic nervous system; creating unusual sensations with subtle stimulation, including immediate feedback; and involving active macro-movement participation.
My thanks go to Robert Schleip for his constructive suggestions and his support of this idea; to Art Riggs and Tom Findley for reading an early draft of this paper and providing useful suggestions; to Penny Robertshawe for editing the manuscript. Three anonymous reviewers and journal editor Chris Moyer provided positive suggestions and valuable comments.
The author declares that there are no conflicts of interest.
Published under the CreativeCommons Attribution NonCommercial-NoDerivs 3.0 License .
a During direct MFR technique, the myofascial tissue restrictive barrier is engaged for the myofascial tissues, and the tissues are loaded with a constant force until tissue release occurs. In contrast, during indirect MFR, the dysfunctional tissues are guided along the path of least resistance until free movement is achieved.(2)
b Somatoemotional release uses fascial unwinding to access a client’s emotions and deals mostly with the physical manifestations of emotional trauma.(1)
Corresponding author: Budiman Minasny, Australian Centre for Precision Agriculture, The University of Sydney, NSW 2006 Australia.
E-mail: b.minasny@usyd.edu.au
INTERNATIONAL JOURNAL OF THERAPEUTIC MASSAGE AND BODYWORK—VOLUME 2, NUMBER 3, SEPTEMBER 2009