The Integrated Taxonomy of Health Care: Classifying Both Complementary and Biomedical Practices Using a Uniform Classification Protocol The Integrated Taxonomy of Health Care: Classifying Both Complementary and Biomedical Practices Using a Uniform Classification Protocol
The Integrated Taxonomy of Health Care: Classifying Both Complementary and Biomedical Practices Using a Uniform Classification Protocol The Integrated Taxonomy of Health Care: Classifying Both Complementary and Biomedical Practices Using a Uniform Classification Protocol Antony Porcino, BSc,1 Colleen MacDougall2
1CAMEO Project, BC Cancer Agency and University of British Columbia, Vancouver, BC, Canada; 2Executive Director and Registrar, Natural Health Practitioners of Canada, Edmonton, AB, Canada.
Background: Since the late 1980s, several taxonomies have been developed to help map and describe the interrelationships of complementary and alternative medicine (CAM) modalities. In these taxonomies, several issues are often incompletely addressed:
- A simple categorization process that clearly isolates a modality to a single conceptual category
- Clear delineation of verticality—that is, a differentiation of scale being observed from individually applied techniques, through modalities (therapies), to whole medical systems
- Recognition of CAM as part of the general field of health care
- Methods: Development of the Integrated Taxonomy of Health Care (ITHC) involved three stages:
- Development of a precise, uniform health glossary
- Analysis of the extant taxonomies
- Use of an iterative process of classifying modalities and medical systems into categories until a failure to singularly classify a modality occurred, requiring a return to the glossary and adjustment of the classifying protocol
Results: A full vertical taxonomy was developed that includes and clearly differentiates between techniques, modalities, domains (clusters of similar modalities), systems of health care (coordinated care system involving multiple modalities), and integrative health care.
Domains are the classical primary focus of taxonomies. The ITHC has eleven domains: chemical/substance-based work, device-based work, soft tissue–focused manipulation, skeletal manipulation, fitness/movement instruction, mind–body integration/classical somatics work, mental/emotional–based work, bio-energy work based on physical manipulation, bio-energy modulation, spiritual-based work, unique assessments. Modalities are assigned to the domains based on the primary mode of interaction with the client, according the literature of the practitioners.
Conclusions: The ITHC has several strengths: little interpretation is used while successfully assigning modalities to single domains; the issue of taxonomic verticality is fully resolved; and the design fully integrates the complementary health care fields of biomedicine and CAM.
KEYWORDS: Complementary therapies, classification; complementary therapies, methods; delivery of health care, integrated; delivery of health care, classification; organizational models interdisciplinary communication
One of the first reviews to discuss health care schemata by medical anthropologists and sociomedical scientists that incorporated complementary and alternative medicine (CAM) was published in 1986. The authors, Levin and Coreil, were focusing on practices of “new age healing.”(1) The reason for developing taxonomies then seems just as pertinent now: to systematically define components of health care. The application of that systematic definition has many relevant uses, from understanding “sociocultural significance and policy implications,”(1) to recognizing how the similarities, differences, and limits of practice relate to each other for practical scenarios such as risk management and clinical decision-making.
Each of the several taxonomies now published is trying to solve a particular need of the developer, usually through a lens shaped by the paradigm of the developer’s approach. For example, Tataryn(2) looks at paradigms of body interaction; Jones(3), at modes of therapeutic action; Grossinger,(4) at historical relationships from an anthropological perspective; and several others from a point of contrast to biomedicine. The need for and development of CAM taxonomies has been dealt with well in other articles; the introduction to the subject by Tataryn(2) is highly recommended. Jones(3) outlines well how a taxonomy is also important to facilitate the communication that is necessary for integrative medicine.
Of the many taxonomies available, the taxonomy of the National Center for Complementary and Alternative Medicine (NCCAM) is the most well known (Appendix 1), in part because it provides a quick overview of the general CAM therapy concepts and how CAM therapies generally relate.(5) However, the categories are so broad that many therapies could be classified under more than one category, yet the process or reasoning of assigning a therapy that fits multiple categories to only one category is not explained. For example, reflexology is often placed under Manipulative and Body-based Practices, while acupressure is placed under Energy Medicine: Biofield Therapies, even though the two are similar in that they both are creating change by manipulation of points on the body to create physical change in other parts of the body (practitioners ascribe different theoretic bases to the two therapies). And while both chiropractic and nuad bo rarn (Thai massage) fall under Manipulative and Body-based Practices, that classification tells little about their actual similarities and differences. No taxonomy system to date has a categorization that fully resolves this issue. Another difficulty exemplified within the NCCAM taxonomy is the lack of verticality, when one category (Whole Medical Systems) is placed at the same conceptual level (horizontally) as other categories that may fall within this supra-category.(6,7) Although a number of taxonomies, such as those by Tatayrn(2) and Jones,(3) were developed to provide more detail about the therapies, none reviewed fully resolved the verticality issue.
Regardless of these shortcomings, taxonomies can be used to solve practical problems. In 2001, the Natural Health Practitioners of Canada (NHPC) had need of a taxonomy for several related purposes:
In addition, the NHPC recognized that a well-conceived taxonomic structure can also give guidance for research because it delineates commonalities among health care approaches. Understanding the common and dissimilar aspects of therapies is important because differing underlying issues within a health care service may have differing research design needs and solutions. For example, a randomized controlled trial works for pharmaceuticals and standardized herbal extracts without much modification, but a randomized controlled trial of reflexology cannot be run in the same way because manual therapies present unique trial research challenges.(8) Reflexology and Swedish massage are both manual therapies, but their underlying concepts of therapeutic action (energy reflex versus physical tissue manipulation) may require different solutions in a research trial, such as different controls or sham treatment. In contrast, research methods for Swedish massage and trigger point therapy can be similar because of the close similarities in the modalities.
None of the taxonomies available provided the needed structure or understanding to resolve the foregoing issues. The primary issues encountered in other taxonomies were these:
A lack of consistent use of language, a lack of verticality, and in many cases, a lack of consideration of how CAM relates to biomedicine all limit the use of the available taxonomies. The NHPC therefore undertook the development of a theory-based taxonomy, grounded in a clear developmental process, that could be used daily for the association’s credentialing and education work and communication with members, businesses, organizations, and governments. The process took five years and involved three stages. The first stage involved the development of a consistent vocabulary; the second, an analysis of various taxonomies detailing the strengths and opportunities; and the third, steps of developing and refining the taxonomy system including consultation with NHPC members.
Development of a vocabulary involved analyzing current language and terminology used by several sources. We reviewed how the CAM community described itself in practitioner writing (magazines, journals, websites) and in discussions with NHPC members and with other CAM organizations. We also reviewed written and verbal sources within the stakeholder community, especially those of governments, researchers, other nonprofit organizations such as the Prince’s Trust and the World Health Organization, and insurance companies. Language choices and definitions were then refined through a consensus process, first by the Credentials Committee of the NHPC, then by the its Board of Directors. Based on issues arising in stage 3, definitions were sometimes refined or altered.
The authors did not have full access to published journals at the time, and so the research process was not fully systematic, but was based on what was available. The references studied provided good coverage of the CAM taxonomies available:
The taxonomic structure was completed and has been used by the NHPC in its current structure since early 2005.
Three additional taxonomies were reviewed as they became available:
During this same period, a number of books undertook the task of describing CAM modalities—from a few to many(11–18). However, these books either used general groupings similar to the NCCAM ideas, groupings by symptoms treated, alphabetic groupings, or no particular pattern. Although they increased public awareness of the many CAM modalities available, these books did not, in our opinion, develop or support a rigorous universal taxonomic approach to understanding CAM services or their relationship with standard health care.
Individual modalities (therapies) were analyzed for distinguishing features and categorized into clusters using the latest version of the classification protocol until conflicts or failure to definitively classify one or more modalities into a single category occurred. The glossary language would be consulted, sometimes refined, and then the classification protocol and developing category definitions would be adjusted and the modalities re-classified in an iterative process. The domains therefore evolved out of the functional clusters that developed.
The process often began with simple yet fundamental questions that arose in the daily work of the NHPC. For example: Is doula work physically or mentally based? Can aerobic workouts at exercise franchise “X” be classified as CAM? Are the classical somatics modalities physically or mentally focused, given their mind–body paradigm of perception?
Such questions were answered through long discussions, usually involving applying various solutions to these questions and testing the effects on other modality classifications. Simultaneously, and in a similar manner, issues of vertical classification were refined. Development predominantly used CAM examples; biomedical examples were used to critique developing answers. Initial classifications and theoretical development were carried out by the authors in collaboration with the NHPC Credentials Committee. The final classification protocol used the primary mode of interaction (primary application or approach) with the client–patient, based on that primary interaction as described in published writings and texts by practitioners acknowledged by other practitioners to be authorities or experts within their discipline.
Assessment: The process of reviewing and evaluating competencies and qualifications. Assessment may also be the initial determination of needs of treatment during a modality session.
Competency component: A specific set of knowledge and skills, and training in applying them.
Complementary and alternative medicine (complementary and alternative health care): A broad range of healing resources that encompass all health systems, modalities, and practices ... other than those intrinsic to the politically dominant health system of a particular society or culture in a given historical period.(19)
Device: Any non-human object used in treatment, ranging from simple technique-assisting objects to machines or electrical stimulators.
Discipline: A discipline level of training includes every competency component needed to safely and appropriately apply the modality on the public.
Domain: Broad-based categories that encompass one or more modalities through the recognition of the primary mode of interaction with the individual
Integrative medicine (integrative health care): any approach that uses a partnering of both biomedicine (Western medicine) and complementary and alternative medicine.
Method: The manner of applying techniques or a way of doing something.
Modality: A modality is a named scope of practice with defined standards of practice.
Named: Having a distinct and unique moniker allowing a modality to be recognized and distinguished from other modalities (for example, Reiki, Feldenkrais Method, massage therapy).
Occupational standards: Skills, knowledge, and abilities required for an occupation as established by a recognized body or through which the qualifications of an individual are assessed.
Primary mode of interaction: While many modalities function, are applied, or can be perceived on more than one level (physical, mental, emotional, spiritual or energetic), there is usually one aspect that defines the overarching approach of practitioners with their patients.
Scope of practice: The scope of practice for an occupation refers to the range of activities that a qualified practitioner of an occupation may practice. It establishes the boundaries of an occupation, especially in relation to other occupations where similar activities may be performed. The scope of practice for an occupation may be established through governing legislation or through internal regulations adopted by a regulatory body.
Specialist:An expert in a special branch of a subject.
Specialization: A specialization level of training requires an appropriate, previously learnt discipline to provide one or more competency components in order to safely and appropriately apply the modality on the public.
Standard for practice: Having a required certification for a given modality, or having recognition or membership with the regulatory body recognized as needed for a given modality.
System: A specified grouping of a number of distinct health care modalities (for example, traditional Chinese medicine, nursing).
Technique: A specific action to achieve a particular outcome (for example, gliding, percussion).
Therapy: A generalized term referring to a specific remedial outcome desired through the application of a modality. When used as part of names, it represents a desire to have the modality considered therapeutic by medical professionals with a Western-medicine paradigm.
The taxonomy of health care (Fig. 1) is a hierarchical structure in which each higher category of health care encompasses the previous level. Thus, domains are groupings of modalities, and modalities (disciplines and specializations) comprise techniques. The most overarching structure is health care, which encompasses any system, modality, or technique that is used as a healing resource. Within this structure, at any given level, all healing resources—biomedicine and CAM— are complementary to each other rather than as compared with biomedicine.
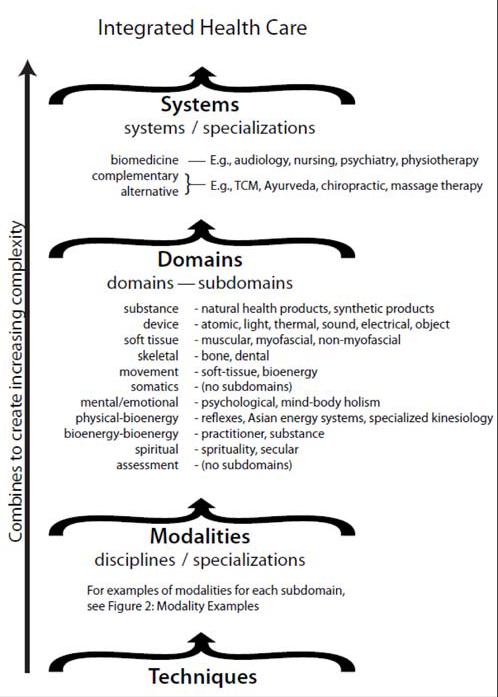
Systems comprise multiple modalities that are consistently taught and used together. For example, physicians and naturopathic doctors both learn multiple ways of approaching health care treatments (prescribing pharmaceuticals or herbs, applying physical manipulations, and using counseling techniques, among others) through training programs that teach to minimum competencies that are fairly uniform throughout North America. “Natural health practitioner” programs train participants in a conglomeration of modalities that can be used together, but, because there is no consistency in the modalities taught in the various programs, that would not be considered a system.
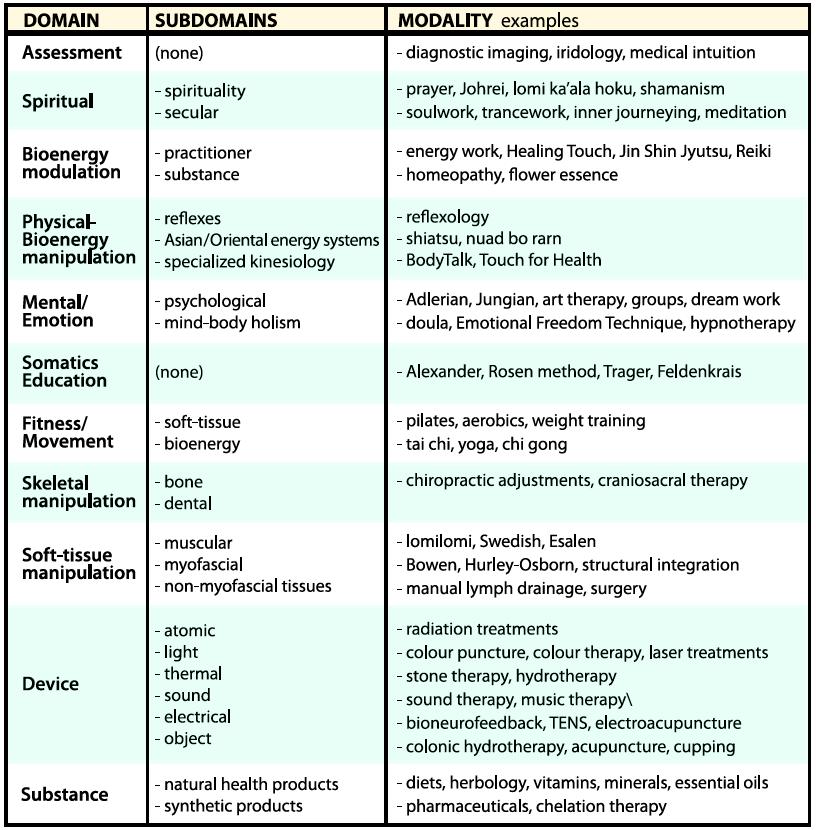
The domain level of the taxonomy of health care is the primary focus of most taxonomies. Here, we summarize the domains and their subdomain categories (Fig. 2 shows examples of modalities for each domain and subdomain):
Fig 2. Modality examples.
Techniques are the building blocks of the entire system. Many techniques are not unique to individual modalities, although how they are taught and used by different modalities may vary. For example, nursing, chiropractic, massage therapy, and shiatsu may all employ a form of gliding (effleurage). Similarly, techniques often cluster, such as different massage stroke types, different assessment techniques for extension and flexion range of motion, or different communication or documentation approaches. Techniques will also cluster into competency components that are recognizable skill sets such as drawing blood (apply tourniquet, raise a vein, sterilize, insert needle, draw blood, remove tourniquet, remove needle, dispose needle, treat puncture, label sample). The application of a technique, such as gliding, is often also a cluster process of techniques (one or more assessments, apply lubricant, perform gliding, communicate with client, evaluate effect), although again, the focus is usually the main technique rather than the pre and post components.
A full taxonomic structure of techniques would be a large undertaking because of the broad scope involved, and it was beyond the purpose for which the present taxonomy was developed. For massage techniques mentioned in this article, we used the massage technique terminology recommended in the taxonomy of massage treatments.(10)
Specializations are a subcategory of systems and modalities. They represent a type of training or practice focus and thus represent another type of dimension that is useful for understanding how training relates to the taxonomy. Specializations involve learning skill sets and knowledge that are more limited in scope and focused on a specific population or on the techniques of applying a specific modality. They are important to a taxonomy because many practitioners identify through their specializations—specialization titles are common within the biomedical system, for example—and it is necessary to clearly see how they fit within the broader discussion of health care and health care nomenclature.
The development of a uniform language was recognized as vital to enable conversation concerning the concepts involved. It is satisfying to see that other researchers are coming to similar conclusions and making inroads within their fields, such as the uniform language of massage techniques.(10) To facilitate communication, we would encourage authors to continue to develop full glossaries for terminology lacking specificity and, as much as possible, to use, in their work, terminology that has been published with clear definitions or that is in line with traditional language use.
The phrase “complementary and alternative medicine” shows some of the difficulties that can arise with terminology. The term is historical and will never have a fully satisfactory meaning both because of its negative definition (it defines what it isn’t, rather than what it is) and because that which is considered standard biomedical care can change over time; for example, psychosocial health determinants are again an important component of health care.(22,23) The chosen definition for CAM acknowledges that, from a North American perspective, CAM and “standard” biomedical health care could be opposite of other cultures in which our standard biomedical care is their “complementary” care—a concept significant to integrative medicine discussions. We prefer the phrase “complementary and alternative health care” (CAHC), rather than CAM, because the term “medicine” is more limited in meaning and nuance: not all health practitioners agree that what they do is “medicine.” However, CAHC is not well known (primarily Canadian), and the current terminology discussions are no longer focused there. Current language concerns are focused on the interpretation of “integrative medicine.” That said, we recognize that CAM is the most familiar acronym and should be interpreted therefore as complementary health care. For similar interpretive reasons, “modality” is preferred to the commonly used “therapy,” because modality respects the perspectives of practitioners who do not consider “therapy” the primary purpose of their work. The recent reuse of the acronym CAM to represent “complementary medicines” and the introduction of CIM (“complementary and integrative medicine”) do not solve any of the inherent biases within the current language. Further, this nomenclature can be interpreted as conceptually disempowering choice or negating inclusion of the alternative, which may imply an inherent North American and biomedicine bias or perspective.
The selection of “integrative medicine” as the top category displays the bias of the society and time in which the definition was produced, in that the definition still requires the split of CAM and biomedicine. The structure of this taxonomy is meant otherwise to emphasize that, in taxonomic conception, there is no difference between the two: all health care modalities and systems are complementary to each other. That is, each has its strengths that complement the strengths of other modalities and systems, and in cases of overlap, the patient has a choice of treatments. Regardless, this definition was chosen because it supports the NHPC’s long-term vision of health care more clearly in terms and concepts as they are used today. As well, many health care providers do not yet perceive CAM on equal footing with biomedicine, and so this taxonomic structure more clearly shows the parallel structure of the two systems. For further exploration of the ongoing development and differing perspectives of integrative medicine, some possible articles to start with include those by Kaptchuk and Miller,(22) Barrett,(24) Bell et al.,(25) and Boon et al.(26,27)
The glossary terms were kept, as much as possible, within the standard use of many of the terms. In some cases, such as in “system,” “discipline,” “domain,” and “specialization,” the standard meanings were kept, but the definitions were made specific to the context of the glossary so that the meaning would be precise enough to enable the taxonomy to work.
The glossary definitions of the taxonomy were altered as the taxonomy was developed. The most significant change was the simplifying of the language—a process that served two purposes:
The definition of “discipline” and “specialization” under “modality” shows this well, because the definitions are consistent with everyday use of the terms, but provide a greater degree of specificity and clarity.
Why were these terms developed?
The people using health care services know the services by modality title (for example, craniosacral therapy), but the discipline and specialization levels serve a practical purpose for those wanting to understand the relationships between various modalities from a credentialing perspective, such as practitioners thinking about training in a modality or a patient wondering about the level of training a practitioner may have. Craniosacral therapy exists as both a discipline and a specialization. The discipline-level programs assume that the practitioner has no other training background or that the programs are designed to fully assume the training of theory and practice from the modality perspective, and thus teach everything—anatomy, physiology, pathology, treatment planning, ethics, file-keeping, hygiene, and client– therapist relationship management—together with the modality’s assessment and treatment protocols. A specialization level of craniosacral therapy, such as that taught in 3- or 4-day workshops, assumes that practitioners have much of this knowledge from other health care modality training, such as massage therapy, and thus the training focuses solely on the modality-specific theory, anatomy, physiology, assessment, and treatment protocols.
The exact designation of a professional specialization is usually controlled by the same credentialing, certifying, or legislative bodies that set training and competency standards for their designated disciplines or systems. An example would be the title that will be used to designate the NCBTMB’s new advanced certification.(28) Specialization as an informal treatment focus (for example, motor vehicle accidents, women) may be controlled by those same bodies or may be more open for the practitioner to use in describing services. The use of such informal practice specializations vary by both profession and jurisdiction. For people or organizations managing practitioner credentials (“assessors”), the use of the discipline and specialization subcategories of a modality or the specialization level of a system enables a fast monitoring of credentialing needs: Any modality or system credential can quickly be verified by an assessor in terms of a practitioner’s competencies held and competencies needed for that practitioner to provide any given specialization. The assessor must therefore have an understanding of the standards that would be appropriate for any given specialization of interest.
The glossary term “named” has a similar basic function. It specifies when something should be included in the taxonomy. Many practitioners can and do train in many modalities. At what point does that combination of treatment practices move beyond being a cluster of treatments to being a title within a taxonomic system? For emerging modalities, it can be a fine line. The two terms used in the definition were “recognized” and “distinguished.” “Recognized” refers to the title being part of common language in a geographic region or within the practitioner’s larger colleague community. “Distinguished” implies that it is unique—something different enough for it to be recognized as distinct from its parent modality or modalities. In naming considerations, this taxonomy does not distinguish between general and proprietary names. Proprietary names are titles that are legal—such as the trademarks Rolfing and Endermologie—or legislative—for example, licensed massage therapist (LMT), registered massage therapist (RMT), and registered nurse (RN).
The glossary, like the taxonomy it is linked with, is a live document for the NHPC in that it will continue to be updated as needed. However, once language was adapted to incorporate the taxonomic verticality and to encompass both CAM and biomedical care in early 2005, it has not since been altered.
The glossary components are useful for their clarification of concepts; however, it is in the context of the full taxonomic structure that the glossary terms should be considered. The taxonomic structure fully solves the issue of verticality: within the structure, systems are a higher order of organization that use the strengths of their multiple modalities and domains in the delivery of health care. This recognition of systems is somewhat different than is often conceived. For example, homeopathy is often called a system because it is a complete health system within itself (theory, production, assessment, and treatment), but within this taxonomic structure it is a modality because it uses a single mode of interaction with patients: administration of a homeopathic remedy that is ingested or topically applied. Conversely, massage therapy is often considered to be a modality because, conceptually, the term “therapy” is often used as if synonymous with “modality.” However, when examined, massage therapy as applied is much more a system, because training encompasses techniques from multiple modalities and multiple domains: Swedish massage; myofascial manipulation, including trigger point work; aromatherapy; hydrotherapy; thermal therapy; and so on. This incorporation of multiple modalities as part of the standard care of massage therapy is becoming common: the National Certification Board for Therapeutic Massage and Bodywork exam requires an understanding of Asian theory and massage practice (energy manipulation through physical massage and chakras),(29,30) and the College of Massage Therapy of British Columbia requires craniosacral therapy and accepts many Asian massage therapy training courses as appropriate continuing education(30).
Within this taxonomy, biomedicine and CAM exhibit similar parallel structure encompassed within integrative medicine. Thus, the taxonomy provides for a consideration of biomedicine simultaneously with, and in the same manner as CAM, using identical criteria. However, the NHPC was focused on solving taxonomic issues of CAM, particularly manual and bio-energy modalities. The parallel structure of CAM and biomedical organization was recognized early in the taxonomic development, and the taxonomy was adapted to be applicable to all health care provision. Although a limited literature search was done, no taxonomic structure of biomedicine was found. It is not known if such a taxonomic or language structure has been fully developed in biomedicine, and how such language would compare to that presented here. Thus the primary caveat with the taxonomic structure lies in the application of glossary terms to biomedicine. That said, this taxonomic structure is fully capable of incorporating biomedicine, and common ideas such as specializations (pediatrics, gynecology, oncology, or surgery, for example) are valid and appropriately expressed within this taxonomic system.
For guiding research, a taxonomic structure establishes a framework for studying ideas and concepts, be they new or historical. Careful examination of the foundational concepts is therefore paramount to ensure that gaps are minimized and conceptual issues are resolved as much as possible. Establishing a clear, uniform, and concise methodologic approach in the development and application of the taxonomic principles to every aspect of the taxonomy ensures consistency and rigor. An iterative review process, combined with careful exploration of possible exceptions to any classification protocol should reveal the taxonomic framework issues. A taxonomy focused only on one health care field, such as those by the Massage Therapy Research Consortium (still under development)(a,b) and the massage therapy taxonomy,(10) may solve localized taxonomic problems and yet cause generalized taxonomic discontinuity. Developing such taxonomies within the context of a larger taxonomic framework ensures that the work not simply benefits the interests of the group designing the taxonomic section, but enables conceptual integration and collaboration across health care fields and a wide variety of taxonomic needs such as understanding therapy concepts and providing research and credentialing guidance.
The domain is the level on which most CAM taxonomic systems are focused, and domains were a primary focus of this taxonomy also. The most difficult and distinguishing feature is how the categories are defined. Past taxonomies have taken various approaches. The most common is to group by superficial features, as NCCAM did, and as many CAM healing books did that used disease or symptom categories to introduce the public to CAM options. Usually, these taxonomies are concerned only with the most common CAM modalities, and so generalization is easy. Others focused on exploring CAM modalities in their variety. They did not try to create a full taxonomic structure, although relationships between some modalities were developed (as listed in “stage 2,” earlier). Fully-developed taxonomies used a theoretic approach to try to encompass the huge varieties of CAM. Tataryn’s approach used paradigms.(2) He set out four categories: body, body–mind, body–energy, body–spirit. Like the NCCAM taxonomy, the Tataryn taxonomy failed to fully resolve individual modalities into single categories and failed to provide practical guidance to people needing a taxonomy for day-to-day work. But the paradigmatic approach that he used is still useful for people not familiar with CAM modalities, because it provides a good basic understanding of the theoretical foundations underlying those modalities. The domains in the present taxonomy could easily be clustered into Tataryn’s groups; their current arrangement proceeds through his four paradigms. In addition, there is value in Tataryn’s argument that understanding the paradigmatic approach to health and disease for each modality is important; the domains proposed here provide that understanding. Jones’ work(3) is the most practical of the taxonomies reviewed and uses a sorting scheme considered also by the NHPC—that of the therapeutic mode of action. The difficulty with that system is that often the action creating the therapeutic effect is not known, and the assumptions or the intention of the practitioner may not resolve the issue. Intention can be fluid, and even change during the course of treatment (as discussed in the massage therapy taxonomy), though it was used as an organizing structure.(10) Near the end of his article, Jones also acknowledges that his system does not fully resolve the issue of what to do when modalities incorporate techniques from different domains or subdomains. The present taxonomy solves that issue by identifying the primary mode of interaction. Focusing on the primary mode of interaction with the patient avoids the difficult issue of intent of the treatment by focusing not on the hoped-for outcome or secondary effects, but on what is happening in the moment of the treatment—for example, using Reiki for pain reduction, with the pain reduction being the secondary outcome of having the patient’s bio-energy field altered. Such focus does not discount possible involvement of other modes of interaction or intent by the practitioners, but recognizes the tendency that there is usually one interaction mode around which the modality’s techniques and theories coalesce and become focused. As well, because the practitioners’ own words about their modalities are used to classify those modalities, only an ability to recognize the paradigm or theoretic constructs of the modalities is required, and not acceptance or understanding. Jones’ article was also one of the first to try to directly deal both with the system issue (though systems were still being classified within domains and had cross-domain conflicts) and with the concept of integrative medicine by incorporating biomedicine modalities within the taxonomy.
The domains of the present taxonomy are based on the primary mode of interaction with the client as described by the practitioners. This largely removes the external examiners’ interpretation of what is known about the modality. The process is simple but takes time. The taxonomist must read through several documents written by authorities (peer-recognized experts) of a modality, focusing both on the theory underlying the modality and on the actual treatment process. The two significant components are thereby identified: the aspect or aspects of the patient that the practitioner is attempting to affect, and how creation of the change is undertaken. These concepts are both clearly outlined for each modality. Rarely is there any ambiguity; most modalities are clear on whether their primary focus is physical, mental, emotional, or spiritual, and how they interact with the patient to achieve the change (treatment). Interactions are usually substance–object; physical manipulation (massage or movement); mental interaction, including verbal and written communication; or bio-energy interaction. The domains represent unique combinations of these processes. The one non-intuitive category is that of unique assessments, which must exist to encompass named modalities that have a distinct theory and primary means of assessment, but do not have a treatment component. This categorization process meets both the transparency and simplicity criteria, though any taxonomist must take the time to learn enough about a modality to know how practitioners define their primary interaction with patients.
There are two competing factors that must be balanced within any taxonomy:
The breadth issue requires weighing the number of categories with the distinctiveness of the categories. Again, the NCCAM system is a good example of giving a broad, simple overview of CAM provision concepts, but its five categories must encompass so much that little is learned or known about the individual modalities within the domains. The present taxonomy has 11 domains, which while being concise, fully differentiate the variants of health care approaches available. Most domains have subcategories that further differentiate important variants on the domain theme, recognizing the diverse range of health care possibilities and the needs of people using a health care taxonomy.
The criteria used to assign modalities to the domains must achieve multiple purposes:
The single-category criterion require categories to be distinct enough that the assignment process can be unambiguous, and the reasons for the boundaries for each domain must be clear. Transparency is important because the reason for the assignment should be clear to anyone who views the modality and the domain, or who could derive the same result without ambiguity. Simplicity is important, because along with transparency, the assignment process should not be onerous either for the taxonomist or for anyone attempting to use or adapt the taxonomy.
The most difficult process encountered was reducing the number of domains to ensure simplicity of use. Such a process is difficult at best, and like past taxonomies, familiarity with a broad range of CAM modalities and convenience were two non-theoretic influences. As an example, consider soft-tissue and skeletal manipulations, which, for credentialing needs and clarity factors, were described as separate domains although both are physical manipulation of a type of body tissue. As well, not all combinations of the aspect of the patient being affected and the approach to creating change (as described above) are represented as separate domains or even as subdomains. Although physical–physical, physical–mental/emotional, physical–bio-energy, mental/emotional–physical, mental/ emotional–mental/emotional, mental/emotional–bioenergy, bio-energy–physical, bio-energy–bio-energy, and spiritual–spiritual are all clearly represented, it is not clear whether modalities involving bio-energy— mental/emotional or the various permutations involving the spiritual perspectives of health—have been developed to any degree. The spiritual domain seems functional as it is; however, other taxonomists may find a need for further definition.
Perhaps the most challenging category was the devices category. Together with the closely related substances category, devices encompasses the “nonhuman” healing vector categories. Devices are any nonhuman object that does not use chemical interaction as the primary mode of interaction. Usually, devices must be licensed by Health Canada (or an equivalent regulatory body), a clue that clearly defines when the device’s own work is the primary focus of the interaction, but something like a massage dibbler (a tool used like a massage therapist’s hand or fingers to provide massage therapy) also falls in this category. When the object is closely tied to another domain, as in the case of acupuncture needles, moxibustion cups, or dibblers, it is important to consider the context of the related field (theory, purpose, focus of the interaction) to fully understand the approach and the related specific training or research needs. For example, traditional Chinese acupuncture holds much in common with tui na or acupressure, including five-element theory and the use of the qi meridian system; medical acupuncture is closer to myofascial approaches in the soft-tissue manipulation domain and would be better understood or researched in the context of that literature and knowledge.
The present taxonomy of integrative health care provides these solutions:
Some might consider eleven domains too complex, but with well over 200 common CAM modalities in North America alone, this system can readily provide an overview of the many relationships between modalities, facilitating comparisons and assisting basic understanding by both the public and health care workers. It resolves many of the outstanding issues identified by previous researchers when developing their taxonomies, particularly issues of verticality and resolution of multiple domain classifications. It removes the paradigm judgments of taxonomists by using the judgments and comments of each modality or system about itself, and avoids the complex issue of treatment intent. It provides a scalable taxonomic structure that easily integrates CAM in a parallel collaborative taxonomic understanding with Western biomedicine. It is hoped that further commentary and participation from the larger community will help to resolve any remaining issues, to flesh out areas that are not as detailed, and to encourage dialogue and better understanding about what each type of health care provider brings to the field of human health care.
The authors thank the members of the NHPC Credentials Committee, who provided feedback and support for the development of this taxonomy on behalf of the organization membership: Matthew van der Giessen, Lori Choma, Tom Lefaive, Tony Corak, Shirley Desborough, Shirley Ann Richards, and Leisa Bellmore.
The authors are not aware of any conflicts of interest with regard to this material.
Published under the CreativeCommons Attribution NonCommercial-NoDerivs 3.0 License .
a Kahn J, Schmidt D, Katomski J. Using a taxonomy of therapeutic massage and bodywork to design massage research protocols. Workshop presented at the North American Research Conference on Complementary and Integrative Medicine; Edmonton, Alberta; May 24–26, 2006.
bKahn J. Manual medicine in the U.S.: overview of use and issues. Presented at the Biology of Manual Medicine Conference; National Institutes of Health, Bethesda, Maryland; June 9, 2005.
The National Center for Complementary and Alternative Medicine (NCCAM)(5) groups complementary and alternative medicine (CAM) practices into four domains, recognizing that some overlap can occur. In addition, NCCAM studies CAM whole medical systems, which cut across all domains.
Whole medical systems are built upon complete systems of theory and practice. Often, these systems have evolved apart from and earlier than the conventional medical approach used in the United States. Examples of whole medical systems that have developed in Western cultures include homeopathic medicine and naturopathic medicine. Examples of systems that have developed in non-Western cultures include traditional Chinese medicine and ayurveda.
Mind–body medicine uses a variety of techniques designed to enhance the mind’s capacity to affect bodily function and symptoms. Some techniques that were considered CAM in the past have become mainstream (for example, patient support groups and cognitive-behavioral therapy). Other mind–body techniques are still considered CAM, including meditation, prayer, mental healing, and therapies that use creative outlets such as art, music, or dance.
Biologically based practices in CAM use substances found in nature, such as herbs, foods, and vitamins. Some examples include dietary supplements, herbal products, and other so-called natural but as yet scientifically unproven therapies (for example, shark cartilage in cancer treatment).
Manipulative and body-based practices in CAM are based on manipulation or movement of one or more parts of the body. Some examples include chiropractic or osteopathic manipulation, and massage.
Energy therapies involve the use of energy fields. They are of two types:
INTERNATIONAL JOURNAL OF THERAPEUTIC MASSAGE AND BODYWORK—VOLUME 2, NUMBER 3, SEPTEMBER 2009