
Figure 1. Clinical classification of patellofemoral pain syndrome (PFPS)(3). VMO = vastus medialis oblique; ML = vastus lateralis.

Massage Therapy Protocol for Post–Anterior Cruciate Ligament Reconstruction Patellofemoral Pain Syndrome: A Case Report
Jennifer Zalta, BS, NCTMB
Jackson, WY, U.S.A.
Background:The intent of the present study was to determine the effectiveness of massage therapy in the rehabilitation of post–anterior cruciate ligament reconstruction patellofemoral pain syndrome. The primary complications following surgical repair of the anterior cruciate ligament—classified as patellofemoral pain syndrome—are hamstring flexion contracture and quadriceps weakness, leading to patellofemoral dysfunction and retropatellar pain.Methods: Treatment included lymphatic drainage, myofascial release, neuromuscular techniques including trigger point release, muscle energy techniques and cross-fiber friction. Orthopedic physical assessment tests were used to chart changes in patellofemoral function and changes in range of motion in the knee during the course of the massage interventions. Subjective reporting on pain level and function were also documented.
Results: A decrease in pain level, hamstring flexion contracture and lateral tracking of the patella were documented.
Conclusion: Massage therapy was determined to be an effective complementary therapy in the treatment of patellofemoral pain syndrome.
KEYWORDS: ACL rehabilitation, retropatellar knee pain, patellofemoral pain syndrome, knee joint flexion contractures, patellofemoral dysfunction
Anterior cruciate ligament (ACL) ruptures are a common athletic injury estimated to occur in 1 of every 3000 people in the United States(1). Surgical reconstruction of the ACL by 4-strand hamstring graft, patellar tendon graft or allograft have proven to be remarkably effective in restoring function and stability to the injured knee. Success rates are high for individuals to return to an active lifestyle after ACL reconstruction, but several complications remain that can limit the individual's full recovery. The three most prevalent complications following ACL reconstruction are quadriceps weakness, flexion contracture of the hamstring muscle group and patellofemoral pain(2).
Patellofemoral pain syndrome (PFPS) has become the "catch-all" diagnosis for the variety of symptoms related to anterior knee pain following ACL reconstruction, including quadriceps weakness, flexion contracture and vastus medialis oblique and vastus lateralis timing dysfunctions(3). Witvrouw et al. concisely charted the clinical classifications of PFPS, as shown in Figure 1(3).
Figure 1. Clinical classification of patellofemoral pain syndrome
(PFPS)(3). VMO = vastus medialis oblique; ML = vastus lateralis.
Flexion contractures are an inability of the collective hamstring muscle group, which includes the biceps femoris, semitendinosus and semimembranosus, to fully lengthen and allow the knee joint to extend. Flexion contracture is traditionally tested and measured by noting heel-height difference with the patient in the prone position. Every 1 cm of heel-height difference correlates with 1 degree of flexion contraction(2).
Multiple studies have shown that ACL injury and ACL reconstruction lead to an increase in bicep femoris activity(4–7). This increase in hamstring activity and contraction prevents anterior translation and limits medial rotation of the tibia, protecting the knee joint from excessive pivoting motion. Injuries to the ACL have been linked to neuromuscular adaptations in the entire leg(8,9). Solomonow et al. found that the increase in hamstring activity that contributes to stabilization of the ACL-deficient knee is a function of an "ACL–hamstring reflex arc"(10). Shelbourne et al. came to similar conclusions, finding that hamstring facilitation was an effective means for stabilizing the ACL-deficient knee during the gait cycle(7). Any decrease in quadriceps force, as found in quadriceps reduction and avoidance patterns, is an effective method for knee stabilization during gait, apart from mid-stance, when the knee nears full extension(11).
Once the ACL has been surgically repaired, this protective reflex to limit medial rotation and anterior tibial translation via hamstring facilitation is no longer necessary. However, the ACL–hamstring reflex arc persists after the ACL has been functionally repaired. For example, in their study on the effects of knee-joint effusion, Torry et al. found that electromyogram (EMG) activity in the biceps femoris, semitendinosus and semimembranosus increased even in the absence of structural instability or joint laxity(8).
Sherrington's Second Law, reciprocal inhibition in muscular contraction, states that when a muscle on one side of a joint is contracted, the muscle on the opposite side of the joint is sent a neurologic signal to relax(12). As Solomonow et al. noted in their study on the ACL-hamstring reflex arc, the hamstring musculature becomes facilitated after an ACL injury(10). Applying Sherrington's Second Law, the quadriceps must become reciprocally inhibited when the hamstrings become neurologically facilitated. Once the ACL is repaired and the hamstring's protective reflex is no longer necessary, the therapist can utilize muscle energy techniques including post-isometric relaxation, contract–relax antagonist–contract, and reciprocal inhibition to normalize the neurologic reflexes of the gastrocnemius, hamstring and quadriceps muscle groups to restore a full range of motion in the knee joint. Shelbourne et al. suggest that restoring full hyperextension as compared with the flexibility of the contralateral knee is crucial in preventing anterior knee pain post ACL reconstruction(7). Prolonged flexion contracture can lead to the development of myofascial trigger points that would result in referred pain, segmented movement and decreased range of motion(13). Myofascial release may be beneficial for any scar tissue or adhesion development within the contracted hamstring muscle group(14).
Weakness in the quadriceps following ACL injury and reconstruction has been noted in numerous studies and has been linked to intra-articular effusion, hamstring facilitation, inhibition of the vastus medialis oblique and neuromuscular recruitment of the hip and ankle muscle groups(2,8,15).
Torry et al. demonstrated that knee joint effusion even in structurally sound knees resulted in neurologic inhibition of the quadriceps(8). The vastus medialis oblique was most significantly affected by the presence of intra-articular swelling; the vastus lateralis and rectus femoris were affected when larger volumes of effusion were present. Torry et al. also noted that, as the rectus femoris became inhibited, the iliopsoas was increasingly recruited to compensate for most of the hip work output(8). Based on that work, lymphatic drainage, when used in conjunction with combined cold and compression techniques such as the AirCast Cryo/Cuff (Aircast, Newark, NJ, U.S.A.), have been hypothesized to possibly have an effect on reducing intra-articular knee effusion and the resulting vastus medialis oblique and quadriceps reflex inhibition.
The function of the vastus medialis oblique in patellofemoral tracking is to prevent lateral subluxation of the patella during knee extension(16–19). The vastus medialis oblique exerts a medial pull on the patella against the lateral pull of the vastus lateralis. The proper timing of the coordinated muscle contraction of the vastus medialis oblique and vastus lateralis is essential for correct patellofemoral tracking. Dysfunctional timing or strength imbalances, or both, between the vastus medialis oblique and the vastus lateralis, as a result of vastus medialis oblique inhibition, can lead to lateral subluxation of the patella, increased patellofemoral contact, retropatellar pain and degeneration of articular cartilage(3,20).
Escamilla et al. studied the effects of flexibility in the hamstrings, gastrocnemius, rectus femoris and iliotibial band, and concluded that a decrease in flexibility negatively affects the biomechanics of the patellofemoral joint(16). Furthermore, Grelsamer stated that patellar malalignment is associated with tightness in the lateral retinaculum, hamstrings, iliotibial band, quadriceps, hip rotators and Achilles tendon(21). In the PFPS client, the primary focus for establishing proper patellofemoral tracking is to increase flexibility in the hamstrings, gastrocnemius, rectus femoris and iliotibial band, and to develop vastus medialis oblique control and strength.
Studies have proposed a correlation between the three most common complications in ACL reconstruction, suggesting that flexion contractures lead to an increase in patellofemoral contact, producing patella irritability and anterior knee pain(2). Intra-articular knee-joint effusion, common in all knee injuries and surgeries, resulted in an inhibitory reflex in the quadriceps, with the vastus medialis oblique showing the most dramatic inhibitory response(8). The vastus medialis oblique is a dynamic stabilizer of the patella, and any delayed or diminished contraction of the vastus medialis oblique can negatively affect alignment of the patella(21). This causal relationship, as shown in Figure 2, demonstrates the importance of postoperative rehabilitation to prevent PFPS development.
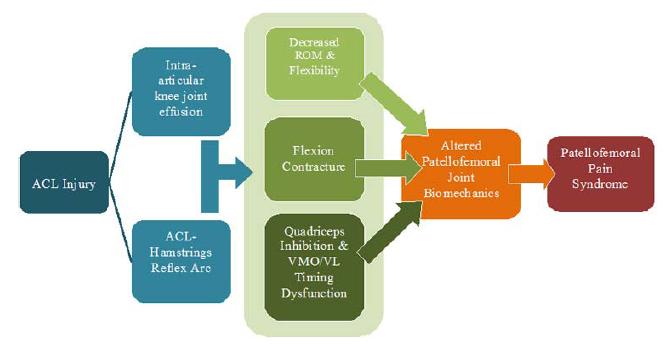
Figure 2. Casual relationship of anterior cruciate ligament (ACL) injury–induced patellofemoral pain syndrome (PFPS). ROM = range
of motion; VMO = vastus medialis oblique; ML = vastus lateralis.
In a literature review using PubMed, keyword searches for ACL reconstruction rehabilitation, anterior knee pain and ACL reconstruction, patellofemoral pain syndrome rehabilitation, retropatellar knee pain, patellofemoral dysfunction, knee joint flexion contracture, massage therapy and orthopedic massage located no published peer-reviewed studies on the effectiveness of integrating massage therapy into the postoperative rehabilitation of ACL reconstruction. Nor were any studies found on the effectiveness of massage therapy for PFPS. The objective of the present case report was therefore to determine the potential role and effectiveness of massage therapy in the post–ACL reconstruction PFPS rehabilitation protocol. Researching the effectiveness of massage therapy may provide a better understanding of PFPS onset following ACL reconstruction and may ultimately improve patient rehabilitation.
A 29-year-old female athlete sustained complete ACL rupture, torn medial meniscus and grade 3 tear of medial collateral ligament of her right knee from a noncontact injury while backcountry skiing. Four days after the injury, subject underwent right-knee ACL reconstruction via hamstring graft and medial meniscectomy with 15% removal. The grade 3 tear of the medial collateral ligament was not surgically repaired. Subject completed a 16-week course of physical therapy post surgery.
The following winter, the subject was unable to return to skiing at pre-injury level or intensity. Subject noted that she had developed a "grinding" sensation in her right knee while ascending and descending stairs and an audible "click" when raising and lowering from a seated position 6 – 7 months post–ACL reconstruction.
One year post–ACL reconstruction, subject returned to physical therapy with lingering retropatellar pain, weakness and "grinding" in the right knee, with audible "click" at 130 degrees extension. One month later, subject was diagnosed with PFPS by the orthopedic surgeon who performed the ACL reconstruction. Subject underwent arthroscopic surgery 4 days later for debridement of patellofemoral cartilage to reduce crepitus and clicking.
The combined ACL–medial collateral ligament–medial meniscus injury sustained by the subject has classically been called the O'Donoghue triad, unhappy triad, injury triad or terrible triad in sports medicine(22,23). Multiple studies have confirmed the common incidence of coupled multi-ligament and meniscus injuries in alpine skiing(24,25). However, these studies reported that ACL–medial collateral ligament–lateral meniscus tears were 9 times more likely to occur than were ACL–medial collateral ligament–medial meniscus tears(23,24).
It is clinically interesting to note that the subject underwent ACL reconstruction 4 days after injury. Shelbourne et al. recommend the importance of proper preoperative care to reduce swelling, restore full hyperextension (compared with the contralateral leg) and to establish extension habits through physical therapy and exercise to reduce the incidence of complications following operative repair(7).
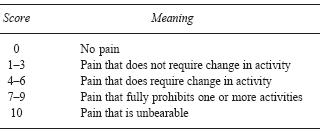
One week before arthroscopic surgery, the subject was seen by a nationally certified massage therapist specializing in orthopedic and sports massage to establish baseline assessment, treatment plan and goals. Subject complained of right knee pain climbing stairs and while raising and lowering from a seated position. Regular physical activities "hurt too much to be fun." Subject was discouraged by audible crepitus and click with flexion and extension of the knee. Pain level 4 was indicated on the functional numeric 0 – 10 pain scale (Table 1).
Table 1 Functional Numerical Pain Scale(26)
Functional goals were established during session 1. The subject's long-term goal was to return to pre-ACL injury activity level and intensity. Subject's short-term functional goals were to return to road biking 2 weeks post arthroscopic surgery and to return to mountain biking 6 weeks post surgery. By 12 weeks post surgery, subject wanted to be able to hike up and down hill pain-free using trekking poles for additional balance and stability.
Active, passive and resisted range of motion were measured with a Baseline HiRes 360-degree, 12-inch plastic goniometer (Fabrication Enterprises, White Plains, NY, U.S.A.) with an International Standards of Measurement (STFR) 1-degree scale. Strength and quality of movement were noted in accordance with the Key to Muscle Grading 0 – 10 scale (10 = normal) outlined by Kendall and McCreary for manual muscle testing (Table 2)(27).
Table 2 The Kendall Key to Muscle
Grading(27)

Four orthopedic physical assessment tests were conducted to evaluate for patellofemoral dysfunction: the active patellar grind test, lateral pull test, step-up test and Waldron test:
The report subject tested positive for patellofemoral dysfunction on the active patellar grind test, step-up test, Waldron test and lateral pull test(28). An audible "click" was observed at approximately 130 degrees of knee flexion and extension in the active range of motion and with resisted range of motion.
An exaggerated Q-angle in flexion (12 degrees) and a positive "bayonet sign" in the right knee were noted with the subject seated and knees flexed to 90 degrees, hip and foot in neutral positioning. Normal Q-angle in seated flexion is 0 degrees. The relevance and reliability of Q-angle measurements in PFPS have been questioned, and therefore little clinical emphasis was given to Q-angle during the present study, beyond noting the bilateral difference in Q-angle measurements between the right and left knees(29).
Using the Kendall Key to Muscle Grading 0 – 10 scale for manual muscle testing, the quadriceps graded at 4, with a gradual release from the test position occurring during range of motion(27). The vastus medialis oblique was visibly atrophied. A soft compact retractable metric tape measure was used to take anthropometric measurements(28) for effusion and atrophy at the following measurement points:
The degree of flexion contracture was measured by heel-height difference evaluation. To measure heel-height difference, the subject is placed in the prone position with thighs supported by the end of the exam table and legs relaxed. The therapist palpates for end feel and measures the difference in heel height, where 1 cm equals 1 degree of flexion contracture(22). The subject's measured heel-height difference signified an 8-degree flexion contracture.
The Ober test was used to determine the potential existence of contractures involving the subject's tensor fasciae latae and iliotibial band. To perform the Ober test, the subject is positioned side-lying on the unaffected side. The inferior leg is flexed at the knee and hip for support and stability of positioning. The therapist passively abducts and extends the subject's superior leg, while keeping the knee in full extension. The therapist slowly lowers the superior leg. Contractures in the tensor fasciae latae and iliotibial band are present if the superior leg remains abducted and does not fall toward the exam table. It is important to abduct the superior leg so that the iliotibial band passes over the greater trochanter. Additionally, the therapist must stabilize the pelvis to prevent posterior rotation during testing(28). A positive Ober test indicated tensor fasciae latae and iliotibial band contractures.
Active trigger points were palpated in the tensor fasciae latae, vastus lateralis and biceps femoris. Fibrous tissue was palpated in the superior lateral aspect of the patella and lateral aspects of the iliotibial band–vastus lateralis border, suggesting a degree of myofascial adhesion.
Nine therapeutic massage sessions were given over a 10-week period that began 4 days post arthroscopic surgery. Massages were scheduled weekly, with 2 sessions during week 3 and no sessions during week 4 because of a conflict in scheduling. Sessions averaged 75 – 90 minutes because this duration allowed for the additional evaluation and discussion that are non-typical in the standard 60-minute wellness massage. All physical assessment evaluations were performed before and after the session. Subjective pain and function level were charted by the subject before and after the session and daily between sessions using the 0 – 10 functional numeric pain scale.
The initial treatment goal was to reduce postsurgical inflammation by lymphatic drainage(30). Once inflammation was managed, the focus shifted to decreasing the hypertonic musculature and increasing the length of the tensor fasciae latae, iliotibial band and hamstring muscle group through muscle energy techniques, including contract–relax antagonist contract–relax, post-isometric relaxation, reciprocal inhibition and myofascial release(30,31). Neuromuscular techniques would be used to deactivate trigger points in the tensor fasciae latae, vastus lateralis and biceps femoris(32). Tender points in the biceps femoris, semitendinosus and semimembranosus were to be addressed with passive positional release. Post-isometric relaxation and contract–relax antagonist–contract were to be used to increase the range of motion in the knee. Fibrotic tissue around the patella would be reduced using myofascial release and cross-fiber friction followed by ice massage to mitigate any potential inflammatory response(30). Ice massage was self-administered for 10 – 15 minutes by the subject, using a frozen paper cup rubbed in a circular fashion around the patella. Strengthening and facilitation of the vastus medialis oblique and hip adductors would be addressed with isometric and eccentric contractions and by self-care exercises (Appendix A) approved by the treating physician(30).
Treatment session 2 was 60 minutes in length, divided into two segments. For the first 15 minutes of the session, the subject discussed the outcome of surgery, her postsurgical progress and her pain level. Active and passive range of motion were evaluated. Resisted range of motion was contraindicated during this session, because subject was non-weight-bearing immediately following surgery. Anthropometric measurements of leg circumference for tracking effusion and atrophy were taken at the joint line and at 5 cm, 10 cm and 15 cm above the patella base using a soft compact metric tape measure. Lymphatic drainage for postsurgical inflammation was performed during the remaining 45 minutes. The subject wore shirt and shorts for each massage to reduce draping time and to aid in mid-session reassessment, which required subject to stand, squat, and take other assessment positions. Sessions 3 – 9 were divided into five 15-minute segments as follows:
Self-Care Recommendations (approved by treating physician): Stationary biking during weeks 1 – 2; road biking after week 2; can begin mountain biking after week 6. Vastus medialis oblique neurologic facilitation: quad sets, wall sits, side-step-ups. Self massage with foam roller for iliotibial band, manual lymphatic drainage, and ice for any swelling. Hamstring stretches with strap.
At completion of the massage therapy series, subject had regained full pain-free range of motion in her knee. Subjective pain levels had been reduced to 0 on the 0 – 10 scale by session 6. Before session 6, when pain level was reported at 0, each session brought a decrease in pain levels post massage (Figure 3).
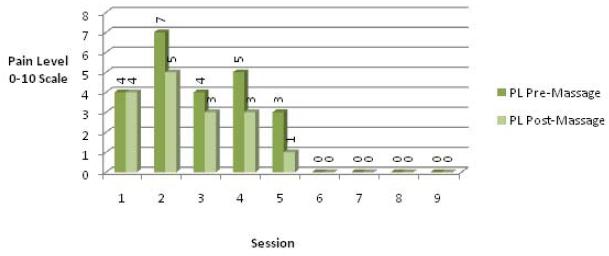
Figure 3. Subject-reported pre- and post-massage pain level (PL) on a 0 – 10 scale for each session. Spikes in pre-massage pain level at
session 2 correspond to postsurgical pain. Session 4 pre-massage pain level was associated with a return to road biking.
Patella tracking, charted using the lateral pull test and Waldron test, showed a diminishing lateral pull. Additionally, the pre-treatment Q-angle, taken in the seated position with knees flexed to 90 degrees, hip and foot in neutral, was approximately 12 degrees as measured with a goniometer. Upon completion of treatment, the Q-angle was approximately 4 degrees. The Ober test for tensor fasciae latae and iliotibial band contracture tested negative by session 5. The active patellar grind test and the side step-up test both registered negative at session 3 (these tests were not conducted during treatment session 2, because subject was not weight-bearing immediately after surgery). Flexion contracture as tracked by heel-height difference showed equal heel heights by the end of session 8 (Figure 4).
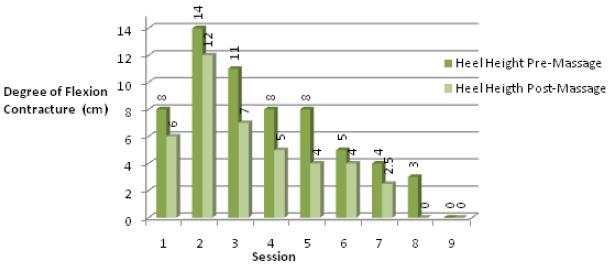
Figure 4. Pre- and post-massage heel-height difference, measuring degree of hamstring flexion contracture.
Anthropometric measurements of knee and distal thigh circumference for tracking effusion and atrophy were insignificantly different, apart from postsurgical inflammation and the effects of lymphatic drainage applied during treatment session 2 (Figure 5).
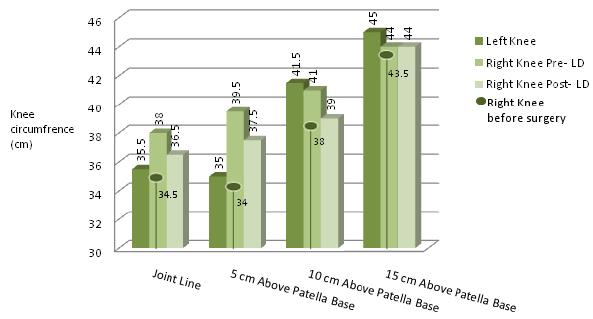
Figure 5. Anthropometric measurements tracking effusion and atrophy pre- and post surgery. Note the decrease in effusion following
application of lymphatic drainage (LD) during session 2. Also note the atrophy of right quadriceps as compared with left quadriceps before surgery.
The results of the present study suggest that massage therapy is an effective complementary therapy in the rehabilitation of post–ACL reconstruction PFPS. Functional goals established by the subject were met within the desired time period. Subject had returned to both road and mountain biking and successfully climbed Grand Teton (4197 m) 14 weeks after arthroscopic surgery for debridement of patellofemoral cartilage.
Massage therapy was effective in reducing subject-reported pain levels after each massage, with a 0 pain level reported after session 6. A 0 pain level was reported through the remainder of the series. Spikes in pre-massage pain level at sessions 2 and 4 corresponded with postsurgical pain and a return to road biking respectively (Figure 3). A clinical correlation was noted between the significant decrease in reported pain level during session 5 and a 4-degree reduction in flexion contracture during the same session.
Session 6 was characterized by a change in Q-angle in seated flexion, with hip and foot in neutral, to 6 degrees from 12 degrees. The increased length in the hamstrings gained in session 5, coupled with focused myofascial release for the iliotibial band and release of active trigger points in the lateral head of the bicep femoris and superior lateral aspect of the gastrocnemius during session 6, potentially helped to reduce Q-angle by allowing the tibia to rotate internally toward a more neutral positioning. Because of the questioned reliability of Q-angle measurements in PFPS assessment, this change in Q-angle during session 6 was regarded as a curiosity rather than a definitive indicator of improvement.
Massage therapy was effective in decreasing the degree of hamstring flexion contracture during each session, and heel-height difference was equalized during session 8 (Figure 4). Lymphatic drainage techniques showed a clinically significant decrease in postsurgical inflammation, reducing knee and distal thigh circumference measurements by as much as 2.75 cm (Figure 6).

Figure 6. (Left panel) Pre– and (right panel) post–lymphatic drainage given 4 days post surgery.
Abnormal patellar tracking was detected in the initial evaluation, with lateral displacement of the patella during extension and quadriceps contraction. This tracking abnormality persisted into session 6, after the debridement surgery, suggesting that the patellofemoral dysfunction was a result of muscular imbalance and not of arthritic changes in the articular surface of the patella. Subject reported that the onset of patella dysfunction symptoms, including retropatellar pain and crepitus, occurred 6 – 7 months after the initial ACL injury and reconstruction surgery. Subject had no history of knee pain before this initial injury, which further suggests that patellofemoral dysfunction was a result of muscular imbalance that was not resolved during the physical therapy after the ACL reconstruction. Crepitus through knee flexion and extension and the "click" at 130 degrees of active and resisted range of motion was resolved largely by debridement of the articular surface of the patella during the arthroscopic surgery and was not detected after session 2.
The subject had reported successful use of self-massage techniques for lymphatic drainage and trigger point release in hamstrings, vastus lateralis and tensor fasciae latae and of stretches and self-care exercises to strengthen and neurologically facilitate the quadriceps. These unmonitored techniques may have influenced the results of this study. Yet self-massage is regularly taught to clients in a therapeutic setting and reflects a realistic scenario. Potential control groups for future research could include participants receiving massage therapy with no self-care exercise and participants receiving self-care-only exercises and no massage intervention.
A 1-year follow-up for this case study yielded only subjective data on pain levels and function because the subject had torn the medial meniscus in the right (studied) knee while playing competitive soccer 2 weeks before the follow-up. Subject indicated that she had experienced no pain before the most recent meniscus tear and had returned to pre–ACL injury activity and intensity.
Despite the positive results, this report has several limitations in tracking quadriceps strength and control. In the absence of electromyogram (EMG) analysis or strength testing equipment, stating the degree of improvement with any certainty is difficult. The present study could benefit from an analysis of quantitative data collected with incorporation of electromyogram analysis of muscle function in the hamstring and quadriceps muscle groups and with incorporation of strength testing results. However, range-of-motion testing suggests improvement in both muscle control and strength: having graded at 4, with painful, weak and segmented movement during session 1, subject improved to grade 10, strong and smooth through the full range of motion, by session 8. Anthropometric measurements for tracking effusion and atrophy in the knee and distal thigh were intended to show an increase in muscle mass as the series progressed, but no significant changes were documented.
Furthermore, this case report serves only as an introductory study of the potential for massage therapy to be incorporated in the PFPS and ACL reconstruction rehabilitation protocols. Single case reports are inherently limited by a small sampling size, lack of a control group, and in this instance, by the lack of adequate testing equipment (EMG, magnetic resonance imaging scans, and radiographs, among other techniques) to verify results(33). No standardization has been brought to rehabilitation of PFPS, and the incorporation of massage protocols into larger-scale studies of the syndrome would be beneficial. Additional research should focus on incorporating massage therapy into the ACL rehabilitation protocol with 1-year follow-up for onset of PFPS and patellofemoral dysfunction. Should future research verify these results, massage therapy could reduce the instance of PFPS and the common complications from ACL reconstruction, including degeneration of the articular surfaces and need for additional surgeries.
1. Miyasaka K, Daniel D, Stone M , Hirshman P. The incidence of knee ligament injuries in the general population. Am J Knee Surg. 1991; 4(1):3–8.
2. Sachs R, Daniel D, Stone M, Garfein R. Patellofemoral problems after anterior cruciate ligament reconstruction. Am J Sports Med. 1989; 17(6):760–765.
3. Witvrouw E, Werner S, Mikkelsen C, Van Tiggelen D, Vanden Berghe L, Cerulli G. Clinical classification of patellofemoral pain syndrome: guidelines for non-operative treatment. Knee Surg Sports Traumatol Arthrosc. 2005; 13(2):122–130.
4. Ciccotti MG, Kerlan RK, Perry J, Pink M. An electromyographic analysis of the knee during functional activities. II. The anterior cruciate ligament-deficient and -reconstructed profiles. Am J Sports Med. 1994; 22(5):651–658.
5. Branch TP, Hunter R, Donath M. Dynamic EMG analysis of anterior cruciate deficient legs with and without bracing during cutting. Am J Sports Med. 1989; 17(1):35–41.
6. Limbird TJ, Shiavi R, Frazer M, Borra H. EMG profiles of knee joint musculature during walking: changes induced by anterior cruciate ligament deficiency. J Orthop Res. 1988; 6:630–638.
7. Shelbourne KD, Lawrance S, Noy R. Prevention of anterior knee pain after anterior cruciate ligament reconstruction. In: Sanchis-Alfonso V, ed. Anterior Knee Pain and Patellar Instability. London, U.K.: Springer; 2006: 283–293.
8. Torry MR, Decker MJ, Viola RW, O'Connor DD, Steadman JR. Intra-articular knee joint effusion induces quadriceps avoidance gait patterns. Clin Biomech (Bristol, Avon). 2000; 15(3):147–159.
9. Berchuck M, Andriacchi TP, Bach BR, Reider B. Gait adaptations by patients who have a deficient anterior cruciate ligament. J Bone Joint Surg Am. 1990; 72(6):871–877.
10. Solomonow M, Baratta R, Zhou BH, Shoji H, Bose W, Beck C, et al. The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. Am J Sports Med. 1987; 15(3):207–213.
11. Shelburne KB, Torry MR, Pandy MG. Effect of muscle compensation on knee instability during ACL-deficient gait. Med Sci Sports Exerc. 2005; 37(4):642–648.
12. Chaitow L, Liebenson C. Muscle Energy Techniques. 2nd ed. Edinburgh, U.K.: Churchill Livingstone; 2001.
13. Chaitow L, Fritz S. A Massage Therapist's Guide to Understanding, Locating and Treating Myofascial Trigger Points. Edinburgh, U.K.: Churchill Livingstone/Elsevier; 2006.
14. Manheim CJ. The Myofascial Release Manual. 3rd ed. Thorofare, NJ: Slack; 2001.
15. Ernst GP, Saliba E, Diduch DR, Hurwitz SR, Ball DW. Lower extremity compensations following anterior cruciate ligament reconstruction. Phys Ther. 2000; 80(3):251–260.
16. Escamilla RF, Fleisig GS, Zheng N, Barrentine SW, Wilk KE, Andrews JR. Biomechanics of the knee during closed kinetic chain and open kinetic chain exercises. Med Sci Sports Exerc. 1998; 30(4):556–569.
17. Knight KL, Martin JA, Londeree BR. EMG comparison of quadriceps femoris activity during knee extension and straight leg raises. Am J Phys Med. 1979; 58(2):57–67.
18. Moller BN, Jurik AG, Tidemand-Dal C, Krebs B, Aaris K. The quadriceps function in patellofemoral disorders. A radiographic and electromyographic study. Arch Orthop Trauma Surg. 1987; 106(3):195–198.
19. Powers CM, Landel R, Perry J. Timing and intensity of vastus muscle activity during functional activities in subjects with and without patellofemoral pain. Phys Ther. 1996; 76(9):946–955.
20. Brody DM. Running injuries. Prevention and management. Clin Symp. 1987; 39(3):1–36.
21. Grelsamer RP. Patellar malalignment. J Bone Joint Surg Am. 2000; 82-A(11):1639–1650.
22. Barber FA. What is the terrible triad? Arthroscopy. 1992; 8(1):19–22.
23. Grana WA. The O'Donoghue triad revisited. Am J Sports Med. 1992; 20(2):238–239.
24. Barber FA. Snow skiing combined anterior cruciate ligament/medial collateral ligament disruptions. Arthroscopy. 1994; 10(1):85–89.
25. Duncan JB, Hunter R, Purnell M, Freeman J. Meniscal injuries associated with acute anterior cruciate ligament tears in alpine skiers. Am J Sports Med. 1995; 23(2):170–172.
26. Hamm M. Impact of massage therapy in the treatment of linked pathologies: scoliosis costovertebral dysfunction and thoracic outlet syndrome. J Bodywork Mov Ther. 2006; 10(1):12–20.
27. Kendall FP, McCreary EK, Provance PG, Rodgers M, Romani W. Muscles: Testing and Function with Posture and Pain. 5th ed. Baltimore, MD: Lippincott Williams and Wilkins; 2005.
28. Magee DJ. Orthopedic Physical Assessment. 4th enhanced ed. St. Louis, MO: Saunders Elsevier; 2006.
29. Greene CC, Edwards TB, Wade MR, Carson EW. Reliability of the quadriceps angle measurement. Am J Knee Surg. 2001; 14(2):97–103.
30. Rattray F, Ludwig L. Clinical Massage Therapy: Understanding, Assessing and Treating Over 70 Conditions. Toronto, ON: Talus; 2000.
31. Hendrickson T. Massage for Orthopedic Conditions. Baltimore, MD: Lippincott Williams and Wilkins; 2003.
32. Travell J, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 2. The Lower Extremities. Baltimore, MD: Williams and Wilkins; 1993.
33. Menard MB. Methodological Issues in the Design and Conduct of Massage Therapy Research. New York, NY: Mosby; 2002.
Corresponding author: Jennifer Zalta, PO Box
214, Jackson, WY 83001 U.S.A.
E-mail: Jen@PeakBodywork.com
Prior to involvement in the study, the subject of this case report was a client of the author's massage therapy practice. The subject gave informed consent when she volunteered for the study. No payment was given to the subject for participation, nor was payment received from the subject for services rendered during the course of the study. The author takes full responsibility for the integrity of the data and the accuracy of the data analysis. Further, the author affirms that this area of potential dual commitment has not influenced the report's objectivity.
Quad Sets: Simply tighten quads when seated or lying down, with knee extended, for a duration of 7 – 10 seconds, repeated 10 times per session, and performed several times daily.
Wall Sits: Stand with back against a wall and knees flexed to 20 – 30 degrees. Squeeze a ball between the knees (to recruit the muscles of the inner thighs). Hold this position for 30 seconds, and increase time as strength increases.
Side-Step-Ups: Beginning with a stair step, stand perpendicular to the stair and step up with the right leg. Watch that the knee is over the heel and in line with the toes. As strength increases, increase the height of the step by using a milk crate, bench, and so on. Perform 3 sets of 10 step-ups a couple of times daily.
Hamstrings: Seated on the floor, with a 6-inch foam roller beneath the knees, press hands down while lifting hips and feet off the floor. Slowly roll hips forward over the foam roller over the entire length of the hamstrings.
Iliotibial Band and Vastus Lateralis: While
seated on the floor with a 6-inch foam roller beneath
knees, roll hips to one side, stacking one leg atop the
other. Press hands down, and lift hips and feet off the
floor. Slowly roll forward and back over the foam roller
from
the superior lateral border of patella to greater
trochanter.
Revolved Triangle: Stand in Mountain Pose. From this position, move feet apart about 3.5 – 4 feet. Raise both arms parallel to the floor and spread them to the sides, shoulder blades wide, palms down. Turn the right foot in, 45 – 60 degrees to the right, and the left foot out, 90 degrees to the right. As you bend to the right side, twist around and bring the left hand to the right ankle or foot, or touch the floor beside the foot (or use a block). The right arm is stretched straight up, perpendicular to the floor, and the head is twisted to gaze at the uplifted right hand. Stay in this position for at least 10 seconds, or for about 3 – 6 breaths, breathing freely. Repeat to the other side.
Supported Hamstring Stretch: In a back-lying position, extend one leg to a comfortable hamstring stretch with strap over ball of foot. Hold for 15 – 30 seconds. Slowly pull strap closer to chest, increasing the hamstring stretch. Repeat for opposite leg. Variation: Bend knee.
Supported Hip and Iliotibial Band Stretch: In a back-lying position, extend one leg to a comfortable hamstring stretch with strap over ball of foot. Slowly lower leg toward the floor across the body. Be sure to keep both shoulders relaxed and touching the floor.