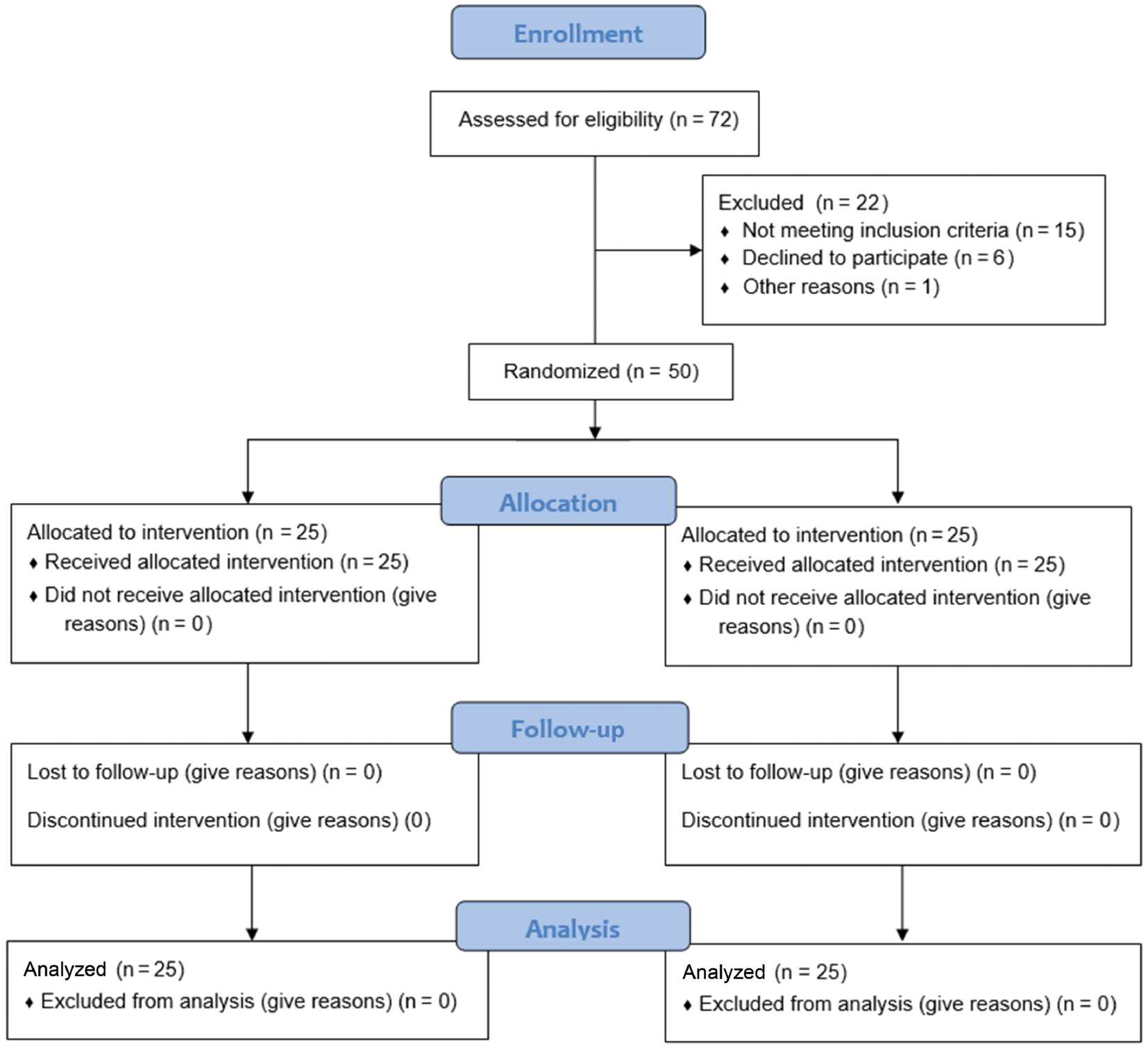
Figure 1. Consort flowchart of extension to randomized pilot and feasibility trials.
| International Journal of Therapeutic Massage and Bodywork (2026) 19(2), 64–73. | https://doi.org/10.3822/ijtmb.v19i2.1285 |
P. Kaviyarasan, BPT1, Sathya Siva, MPT1*, Sukumar Ramaswami, M.D2, F. Khizar Husin, BPT1, D. Hareeshankar, BPT1, A. Fayaz, BPT1, Prathap Suganthirababu, PhD1
1Department of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India
2Department of Radiology, Saveetha Institute of Medical and Technical Sciences, Chennai, India
Background: Myofascial trigger points (MTrPs) in the rhomboid muscles contribute to pain, muscle tightness, and restricted movement, impacting quality of life. Various interventions, including myofascial release (MFR) and isometric relaxation (IR), have been used to alleviate symptoms.
Aim: This pilot study aims to explore the feasibility and preliminary efficacy of MFR combined with active stretching versus IR combined with active stretching in the management of rhomboid MTrPs, with the goal of informing the design of future full-scale studies.
Methods: A randomized controlled trial was conducted with 50 participants diagnosed with rhomboid MTrPs. Participants were assigned to two groups: group A (MFR with active stretching) and group B (IR with active stretching). Interventions were administered for 4 weeks (five sessions per week). Pre- and post-intervention assessments were conducted using the Numerical Pain Rating Scale (NPRS) and goniometric measurements of range of motion (ROM). Statistical analysis was performed using the Wilcoxon method and Mann–Whitney U test via SPSS version 27.
Results: After 4 weeks, group A showed a statistically and clinically significant reduction in NPRS scores from 7.28 ± 0.737 to 5.28 ± 1.061 (p < 0.001, r = 0.59), exceeding the established minimal clinically important difference (MCID) of 2 points for the NPRS. In contrast, group B showed a smaller reduction from 7.16 ± 0.800 to 6.44 ± 1.003 (p < 0.001, r = 0.57), which, although statistically significant, did not meet the MCID threshold, suggesting limited clinical relevance. Similarly, ROM improved in group A from 47.16 ± 1.675 to 52.12 ± 1.616 (p < 0.001, r = 0.63) and in group B from 47.36 ± 1.777 to 48.88 ± 2.147 (p < 0.001, r = 0.56). Group A demonstrated greater improvement in both pain reduction and mobility.
Conclusion: This study concluded that both treatments were successful in addressing rhomboid trigger points. MFR combined with active stretching demonstrated greater pain reduction and improved flexibility. These findings suggest MFR with active stretching may be a valuable addition to clinical health practice guidelines for managing rhomboid trigger points.
KEYWORDS: Isometric relaxation; myofascial release technique; randomized controlled trial; rhomboids; World Health Organization
A myofascial trigger point (MTrP), sometimes referred to as a trigger point, is an irritable point that is usually found in the muscle fascia or within a taut skeletal muscle band. The disorder is characterized by discomfort and restricted movement resulting from the constriction of these trigger points.(1) MTrPs may play a role in the onset and maintenance of various conditions, which have multiple contributory components and complex etiologies.(2)
MTrPs are believed to develop due to factors such as postural imbalance, psychological stress, muscle overuse, or repetitive strain injuries. According to Srbely et al., an “energy crisis” involving adenosine triphosphate (ATP) depletion may occur within the muscle, leading to sustained contracture and reduced capillary circulation, which creates a hypoxic environment that impairs normal muscle relaxation. Myofascial pain is highly prevalent, affecting approximately 85% of individuals at some point in their lives. It contributes significantly to musculoskeletal discomfort worldwide, with neck and upper back pain being among the most commonly reported complaints. Rhomboid MTrPs in particular can lead to restricted shoulder movement and persistent upper back pain and a reduced quality of life, underscoring the need for effective treatment strategies.(3–6)
Myofascial release (MFR) is a method for mobilizing soft tissues. This phenomenon is characterized by “myofascial system-mediated interfaces that provide mechanical, neurological, and psycho-physiological adaptive potential.”(7–10) MFR therapy manipulates the myofascial complex using precisely guided low-load, long-duration mechanical pressures with the goals of restoring optimum length, reducing discomfort, and enhancing function.(11) MFR breaks down adhesions by using manual traction and extended muscle and fascia stretching, which reduces discomfort and improves flexibility, thereby increasing the range of motion (ROM).(12) Myofascial practitioners, according to Stanborough, believe that pressure on pain-sensitive tissues like blood vessels and nerves can be reduced by reestablishing the length and health of constricted connective tissue. The two most common methods of MFR use are the direct technique and the indirect technique.(13) Active stretching, on the other hand, encourages flexibility and relaxation by having the patient actively move a muscle into a stretched posture. Clinical practice has employed both strategies to treat MTrPs; however, little research has been done on the effectiveness of MFR and active stretching together, particularly for rhomboid MTrPs.(14,15)
Despite the clinical relevance of MFR and active stretching in treating MTrPs, a significant gap exists in the literature regarding their combined use, particularly when compared with other commonly used interventions, such as isometric relaxation (IR) techniques. Previous studies have primarily focused on isolated techniques or examined other muscle groups, leaving a lack of data specific to the rhomboid region. Furthermore, few head-to-head comparisons exist evaluating the relative efficacy of MFR and IR, both in conjunction with active stretching. This study addresses this gap by investigating the comparative effectiveness of MFR versus IR techniques, each combined with active stretching, in the management of rhomboid MTrPs. By providing direct evidence on the relative benefits of these interventions, the findings may help inform and refine clinical strategies for a more targeted and effective treatment of rhomboid trigger points.
The primary objectives of this study were to determine the effectiveness of the MFR technique combined with active stretching in reducing pain and improving functional activity and to assess the effectiveness of IR combined with active stretching in achieving similar outcomes. The secondary objective was to analyze and compare the overall efficacy of both intervention approaches in treating rhomboid MTrPs.
This research was conducted as a pilot randomized controlled trial. Ethical approval was granted by the Institutional Scientific Review Board of Saveetha Institute of Medical and Technical Sciences, Chennai, India, with the approval number 417/07/2024/ISRB/UGSR/SCPT. The study adhered to the guidelines outlined in the CONSORT 2010 statement: extension for randomized pilot and feasibility trials (refer to Figure 1).
Figure 1. Consort flowchart of extension to randomized pilot and feasibility trials.
The research question was confirmed with the FINER criteria (Feasible: a pilot study is appropriate to test the methods and assess practicality in terms of participants and resources; Interesting: it addresses a common issue—rhomboid trigger points—and compares two therapeutic techniques, which could inform clinical practice; Novel: comparing of MFR and IR with active stretching; Ethical: ethical approval and informed consent will ensure participant safety and well-being; Relevant: the study is highly relevant to physical therapy, with potential to improve treatment choices for trigger points) and framed using the PICO criteria (Population, Intervention, Comparison, Outcome).
P—patients with rhomboid trigger points.
I—MFR combined with an active stretching protocol.
C—comparing MFR combined with active stretching versus IR combined with active stretching.
O—Numerical Pain Rating Scale (NPRS), goniometer.
Research question statement
This pilot study was conducted in the Physiotherapy Department at Saveetha Hospital, Chennai, India, over a 6-week period from the second week of August to the third week of September. A total of 50 participants were selected using a simple random sampling technique from the staff of Saveetha Institute, including personnel from the reception, information technology, and building maintenance departments who met the inclusion criteria.
Participants aged 18–65 years, of both genders, were eligible for inclusion if they presented with localized pain in the rhomboid muscle region, specifically between the scapula and the spine. The presence of MTrPs was confirmed through physical examination, which included palpation for taut bands, localized tenderness, and reproduction of referred pain patterns characteristic of rhomboid trigger points. Additional inclusion criteria included acute pain lasting <3 months and a pain score ranging from 5 to 8 on the NPRS. Participants were excluded if they had a history of upper back surgery, neurological disorders such as cervical radiculopathy, were currently using pain medication, had skin infections or dermatological conditions that could interfere with treatment, or had cognitive impairments that could hinder participation or the ability to provide informed consent.
Eligible individuals were assigned unique identification numbers and randomly selected using a computer-generated method via Microsoft Excel’s RAND function to ensure unbiased participant selection and allocation. Written informed consent was obtained from all participants prior to their inclusion in the study.
The sample size of 50 participants (25 per group) was chosen based on recommendations for pilot and feasibility studies, which commonly suggest enrolling 24–50 participants.(16) This number was considered adequate to allow for a preliminary evaluation of intervention effects, estimation of variability, and assessment of recruitment and retention procedures.(16) The study aimed to explore the feasibility and preliminary efficacy of MFR combined with active stretching versus IR combined with active stretching in the management of rhomboid MTrPs, to inform the design of future full-scale studies.
Participants were randomly divided into two equal groups (n = 25 each) using a computer-generated randomization method. Group A received the MFR technique combined with active stretching, while group B received IR combined with active stretching. The stretching protocol included exercises such as the scapular protraction stretch, dynamic hug stretch, standing wall stretch, and seated upper back stretch. Baseline demographic data were collected from all participants before the commencement of the intervention (Table 1).
Table 1. Subject Demographics
| Category | Subcategory | Number of Participants |
|---|---|---|
| Gender | Male | 29 |
| Female | 21 | |
| Age, years | 18–25 | 25 |
| 26–50 | 15 | |
| 51–65 | 10 | |
| Comorbidities | Diabetes mellitus | 16 |
| Hypertension | 14 | |
| Thyroid | 0 |
The study population included subjects who experienced discomfort in the rhomboids, as determined by the inclusion and exclusion criteria. Informed consent was obtained after the study procedure was explained. The subjects were allocated into two groups: group A received MFR with active stretching, while group B received the IR exercise with active stretching. Both groups received an intervention. Pre- and post-test outcome measures were analyzed.
Group A
In this group, the subject received MFR technique combined with active stretching, administered by a physiotherapist with 5 years of experience. The treatment procedure is described below.
The MFR technique was performed in three cycles per session, with each participant receiving five sessions per week over a 4-week period.(1)
To release a rhomboid trigger point, the patient was prone on a treatment table or sitting upright, depending on their comfort and accessibility to the affected area. The therapist began by palpating the rhomboid muscles, located between the scapulae and the spine, to identify taut bands or hypersensitive areas. The diagnosis of an MTrP was based on the criteria described by Simons et al., which include the presence of a taut band within the muscle, a hypersensitive tender spot within that band, reproduction of the patient’s referred pain pattern upon palpation, and a local twitch response. These features together distinguish a trigger point from a simple tender point. Once located, firm and sustained pressure is applied using fingers, knuckles, or an elbow, gradually increasing to a tolerable level for the patient. The therapist guided the patient through slow scapular movements, such as protraction and retraction, or gently moved the patient’s arm to stretch the rhomboids while maintaining pressure. The pressure was held for 20–30 s or until the tension started to release, then gradually reduced. This process was repeated three times to address different trigger points if necessary. A 1-min rest was given between each cycle.(1)
Active stretching was administered in three sets per session, with five sessions conducted each week over a period of 4 weeks.(17)
Scapular protraction stretch: The subject began in a seated or standing position. The arms were extended forward at shoulder height, with fingers interlocked or one hand placed over the other. The subject pushed the arms away from the body while rounding the upper back, allowing the shoulder blades to move apart (protraction). The chin was kept slightly tucked and the stretch was held for 20–30 s. This was repeated three times, with 30 s of rest given after each repetition.
Dynamic hug stretch: The subject stood or sat upright, with arms extended out to the sides at shoulder height. The arms were slowly brought forward in a sweeping motion, crossing one arm over the other at chest level. A stretch was felt in the upper back and between the shoulder blades. The arms were then released and returned to the starting position, alternating which arm crossed over the other with each repetition. Three slow, controlled repetitions were performed, with 30 s of rest given after each repetition.
Standing wall stretch: The subject faced a wall and placed their hands on it at shoulder height, keeping the arms straight. They slowly stepped back, leaning their torso forward while keeping their hands firmly planted on the wall. The chest was lowered, allowing the shoulder blades to stretch apart gently. This position was held for 20–30 s, ensuring the head remained in line with the spine. The stretch was repeated three times, with 30 s of rest given after each repetition.
Seated upper back stretch: The subject sat on a chair, crossed the arms in front, and rested the hands on opposite shoulders or hugged the torso. They leaned forward slightly, rounding the upper back while tucking the chin to the chest. A stretch was felt along the upper back and between the shoulder blades. The stretch was held for 20–30 s before returning to an upright position. This was repeated three times, with 30 s of rest given after each repetition.
Group B
In this group, the subject underwent IR combined with active stretching, administered by a physiotherapist with 5 years of clinical experience. The treatment procedure is outlined below.
IR was performed in three sets per session, with five sessions per week over a 4-week period.(17)
The patient performed an isometric contraction of the affected muscle (in this case, the rhomboid), meaning the muscle is engaged without changing its length. This contraction is usually maintained for approximately 5–10 s. PIR is then facilitated, typically by applying a counterforce provided by the therapist. After the contraction, the muscle is allowed to relax completely. This relaxation phase helps reduce muscle tension and alleviate discomfort associated with trigger points. The contraction and relaxation cycle was repeated several times, often three to five repetitions, to achieve optimal results. A 1-min rest was given between each set.
Active stretching for this group was performed according to the same protocol used for group A.
Outcome measure: All subjects were assessed using the NPRS and goniometer, both before and after the intervention (first day and after 4 weeks of intervention). The outcome measures were administered by a trained physiotherapist who was blinded to the group allocation to reduce assessment bias.
The NPRS is a widely used tool for assessing the level of pain that patients, particularly those with chronic conditions, are experiencing. This scale typically takes the form of a horizontal line with numbers ranging from 0 to 10. From 0 (no pain) to 10 (the most agonizing anguish possible), each number indicates a different degree of pain intensity. When given a time period, often the last 24 h, subjects are asked to select the number that best captures their level of pain at that time. The NPRS is favored as a universal instrument for assessing the degree of pain due to its ease of use and simplicity, even if its primary focus is on measuring pain rather than discussing its qualitative characteristics. The minimal clinically important difference (MCID) for the NPRS is 2 points, meaning a change of 2 or more points is considered clinically significant (Ranzatto et al.).(18)
A goniometer is a device used to measure the ROM of joints, providing essential data for assessing joint function and guiding rehabilitation. In this study, a goniometer was used to measure shoulder elevation in the scapular plane (scaption). The patient was instructed to raise the arm in the scapular plane—approximately 30–45° anterior to the frontal plane—while keeping the elbow extended. The axis of the goniometer was positioned at the lateral acromion, with the stationary arm aligned with the thorax and the moving arm aligned with the humerus. All goniometric measurements were taken by a physiotherapist with 5 years of clinical experience, who was blinded to the group allocation to minimize bias. This measurement technique for scaption is considered highly reliable. According to Kolber et al., goniometric assessment of scapular plane shoulder elevation demonstrates excellent intra-rater reliability (intraclass correlation coefficient >0.90), making it a valid and consistent method for clinical and research settings.(19)
This study was conducted on 50 subjects with two groups: group A (experimental) and group B (comparison). Each group received different interventions. The groups were compared using NPRS and ROM scores analyzed with the Wilcoxon test (Table 2). The difference between NPRS and ROM between pre and post-test was assessed using the Mann–Whitney U test in SPSS version 27.
Table 2. Comparison of NPRS and ROM Within Group A and Group B
| NPRS Outcome | Pre-Test Mean ± SD |
Post-Test Mean ± SD |
Z-value | p-Value |
|---|---|---|---|---|
| Group A (N = 25) | 7.28 ± 0.737 | 5.28 ± 1.061 | −4.187 | <0.001 |
| Group B (N = 25) | 7.16 ± 0.800 | 6.44 ± 1.003 | −4.025 | <0.001 |
| ROM Outcome | Pre-Test Mean ± SD |
Post-Test Mean ± SD |
Z-value | p-Value |
| Group A (N = 25) | 47.16 ± 1.675 | 52.12 ± 1.616 | −4.441 | <0.001 |
| Group B (N = 25) | 47.36 ± 1.777 | 48.88 ± 2.147 | −3.992 | <0.001 |
Z values derived from the Wilcoxon signed-rank test.
p < 0.05 considered statistically significant.
NPRS = numerical pain rating scale; ROM = range of motion (measured in degrees); SD = standard deviation.
The outcomes of the study were evaluated following a 4-week intervention period. No adverse effects or complications were reported in either group throughout the study period. Adverse events were monitored through participant self-report and clinical observation at each weekly session.
Group A showed a significant reduction in NPRS scores from 7.28 ± 0.737 (pre-test) to 5.28 ± 1.061 (post-test), with a Z-value = −4.187, p < 0.001, and a 95% confidence interval (CI) (1.58–2.22), indicating a statistically and clinically significant reduction in pain. Group B showed a moderate reduction in NPRS scores, from 7.16 ± 0.80 to 6.44 ± 1.00, with a Z-score of −4.025, p < 0.001, and a 95% CI (0.55–0.94). This reduction was statistically significant, although less pronounced than that in group A (Table 2).
The combined NPRS comparison (Table 3) shows that the overall mean NPRS decreased from 7.22 ± 0.764 to 5.86 ± 1.178, with Z = −3.508, p < 0.001, 95% CI (0.88–1.73), indicating a statistically significant improvement.
Table 3. Difference in NPRS and ROM Between Pre- and Post-test
| NPRS | Mean ± SD | Z-value | W | U | p-Value | r-Value |
|---|---|---|---|---|---|---|
| Pre-test | 7.22 ± 0.764 | −0.512 | 613 | 288.00 | 0.609 | 0.072 |
| Post-test | 5.86 ± 1.178 | −3.508 | 462 | 137.5 | <0.001 | 0.496 |
| ROM | Mean ± SD | Z-value | W | U | p-Value | r-Value |
| Pre-test | 47.26 ± 1.712 | −0.423 | 616 | 291.00 | 0.672 | 195.195 |
| Post-test | 50.50 ± 2.493 | −2.678 | 399.5 | 74.50 | <0.001 | 143.245 |
Z values from the Wilcoxon signed-rank test.
W and U are test statistics.
p < 0.05 considered statistically significant.
r-value represents the effect size.
NPRS = numerical pain rating scale; ROM = range of motion (measured in degrees); SD = standard deviation.
Group A improved significantly from 47.16 ± 1.675 to 52.12 ± 1.616 with Z = −4.441, p < 0.001, and a 95% CI (4.48–5.31), reflecting a notable gain in shoulder mobility (Table 2). Group B showed a smaller improvement from 47.36 ± 1.777 to 48.88 ± 2.147, with Z = −3.992, p < 0.001, and a 95% CI (1.09–1.68), suggesting a slight but statistically significant increase in mobility.
The combined ROM comparison (Table 3) shows that the mean ROM increased from 47.26 ± 1.71 to 50.50 ± 2.49, with a Z-score of −2.678, p < 0.001, and a 95% CI of (2.63–3.45), demonstrating an overall improvement in shoulder elevation range.
The effectiveness of MFR and IR in conjunction with active stretching was compared for the treatment of rhomboid MTrPs in this study. The outcomes demonstrated that while both treatments considerably decreased pain and enhanced ROM, MFR combined with active stretching offered the best pain alleviation and flexibility improvements. A limited sample size and a brief intervention period were two study constraints that may have affected the generalizability of the results, even though the results suggest that MFR is a more successful strategy. To validate the long-term advantages, future studies should utilize larger sample sizes, longer follow-up periods, and objective tests, such as electromyography. Clinically, MFR combined with active stretching may be a preferred intervention for managing rhomboid trigger points due to its greater effectiveness in pain reduction and ROM improvement.(4) MTrPs in the rhomboid muscles are common sources of pain and dysfunction, often associated with poor posture, repetitive strain, or muscular imbalances. Various therapeutic approaches are employed to alleviate pain, restore function, and improve muscle flexibility. Two commonly used methods are MFR with active stretching and IR with active stretching. This discussion compares these two interventions in terms of their efficacy for managing rhomboid trigger points. According to Moylan et al., MFR can significantly reduce pain intensity and improve functional movement in patients with MTrPs. This approach specifically targets the muscle knots and tight fascia that cause discomfort associated with MTrPs.(20) Lee et al. demonstrated that MFR effectively provides immediate relief for myofascial pain syndrome by addressing restrictions in the fascia and improving blood flow to the affected regions. They also noted that pairing MFR with active stretching further improves treatment outcomes by helping to preserve muscle flexibility following the therapy. In our pilot study, we compared this combined approach of MFR and active stretching with a treatment involving IR followed by stretching therapy.(21) Simons and Travell explored the effectiveness of IR techniques and found them to be effective in reducing muscle spasm and alleviating pain associated with MTrPs. The relaxation phase following the isometric contraction allows the muscle fibers to release tightness, improving flexibility.(22) Mikalauskas and Laurinavicius demonstrated that incorporating IR with stretching significantly improved both muscle flexibility and functional movement in patients with upper back pain. In rhomboid trigger points, this combination has been shown to effectively reduce the discomfort and stiffness associated with formation, improving the ROM and reducing the recurrence of pain.(17) Mcarthur conducted a study comparing IR with active stretching against other forms of treatment and found that this combined technique produced superior outcomes in managing myofascial pain, especially in patients with upper back and shoulder pain.(23) Khan et al. found that both MFR and IR resulted in significant pain reduction and increased ROM in patients with non-specific neck pain points.(24)
While MFR and IR combined with active stretching are generally safe interventions for managing rhomboid trigger points, certain contraindications must be considered. MFR should be avoided in cases of acute inflammation, open wounds, skin infections, or fractures in the treatment area to prevent exacerbation of symptoms or tissue damage. Similarly, IR exercises may not be suitable for patients with severe muscle weakness, recent surgery, or certain cardiovascular conditions where increased muscle tension could pose risks. It is essential to screen patients carefully to ensure these interventions are applied safely, minimizing the risk of adverse effects while maximizing therapeutic benefits.(1,2,25–29)
In conclusion, both MFR with active stretching and IR with active stretching are effective in managing rhomboid trigger points by reducing pain and improving function. However, the combination of MFR with active stretching showed superior results in terms of pain relief and flexibility, compared to IR with active stretching.
From a clinical perspective, incorporating MFR with active stretching into treatment protocols is recommended for patients presenting with myofascial dysfunction, particularly those experiencing postural imbalances, overuse injuries, or sedentary lifestyles that commonly lead to rhomboid trigger points. This approach may be especially beneficial in outpatient musculoskeletal therapy settings, sports rehabilitation, and among individuals such as office workers, athletes, or manual laborers. However, clinicians should exercise caution when applying MFR techniques to individuals with contraindications such as acute inflammation, fractures, bleeding disorders, or severe osteoporosis.
Tailoring interventions to the patient’s specific condition and tolerance levels is essential to ensure safety and optimize outcomes. By thoughtfully integrating MFR with active stretching into therapeutic strategies, clinicians can enhance pain management and functional recovery in patients with rhomboid trigger points and related myofascial pain syndromes.
The limitations of the study include a small sample size, which reduces the ability to generalize the findings. Additionally, the study lacks long-term follow-up, making it difficult to assess the sustained effects of the interventions over time.
For future research, it is recommended to use a larger sample size to enhance statistical power and generalizability. Long-term follow-up assessments should be incorporated to evaluate the durability of the effects, and a more diverse participant group should be included to ensure broader applicability.
The authors declare there are no conflicts of interest.
No sources of funding were used in this study.
Study design/planning: Kaviyarasan P, Sathya Siva,Sukumar Ramaswami,Prathap Suganthirababu. Data collection/entry: Hareeshankar D, Fayaz A. Data analysis/statistics: Sathya Siva. Data interpretation: Sathya Siva, Prathap Suganthirababu. Preparation of manuscript: Khizar Husin F, Sathya Siva. Literature analysis/search: Hareeshankar D, Fayaz A.
1. Simons DG, Travel JG, Simons LS. Myofascial Pain and Dysfunction: The Trigger Point Manual. Upper Half of Body. 2nd ed. Williams and Wilkins; 1999.
2. Sergienko S, Kalichman L. Myofascial origin of shoulder pain: a literature review. J Bodyw Mov Ther. 2015;19(1):91–101. [CrossRef] [PubMed]
3. Bron C, Dommerholt JD. Etiology of myofascial trigger points. Curr Pain Headache Rep. 2012;16(5):439–444. [CrossRef] [PubMed]
4. Hong CZ, Simons DG. Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch Phys Med Rehabil. 1998;79(7):863–872. [CrossRef] [PubMed]
5. Shah JP, Gilliams EA. Uncovering the biochemical milieu of myofascial trigger points using in vivo microdialysis: an application of muscle pain concepts to myofascial pain syndrome. J Bodyw Mov Ther. 2008;12(4):371–384. [CrossRef] [PubMed]
6. Srbely JZ, Dickey JP, Bent LR, Lee D, Lowerison M. Capsaicin-induced central sensitization evokes segmental increases in trigger point sensitivity in humans. J Pain. 2010;11(7):636–643. [CrossRef] [PubMed]
7. Nambi G, Alghadier M, Khanam H, Pakkir Mohamed SH, Aldhafian OR, Alshahrani NA, et al. An additive effect of instrument-assisted soft tissue mobilization with spinal manipulation in cervicogenic headache: a randomized controlled trial. Pain Ther. 2024;13(6):1679–1693. [CrossRef] [PubMed]
8. Hoy D, March L, Brooks P, Blyth F, Woolf A, Bain C, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. [CrossRef] [PubMed]
9. Skootsky SA, Jaeger B, Oye RK. Prevalence of myofascial pain in general internal medicine practice. West J Med. 1989;151(2):157–160. [PubMed]
10. Chaudhary ES, Shah N, Vyas N, Khuman R, Chavda D, Nambi G. Comparative study of myofascial release and cold pack in upper trapezius spasm. Int J Health Sci Res. 2013;3(12):20–27.
11. Manheim CJ. The Myofascial Release Manual. 4th ed. Slack Incorporated; 2008.
12. Altindag O, Ozaslan S. Efficacy of myofascial release method on pain and disease severity in patients with fibromyalgia. J Pain Relief. 2014;3:161. [CrossRef]
13. Stanborough M. Direct Release Myofascial Technique: An Illustrated Guide for Practitioners. Churchill Livingstone; 2004.
14. Feland JB, Myrer JW, Schulthies SS, Fellingham GW, Measom GW. The effect of duration of stretching of the hamstring muscle group for increasing range of motion in people aged 65 years or older. Phys Ther. 2001;81(5):1110–1117. [CrossRef] [PubMed]
15. Hanten WP, Olson SL, Butts NL, Nowicki AL. Effectiveness of a home program of ischemic pressure followed by sustained stretch for treatment of myofascial trigger points. Phys Ther. 2000;80(10):997–1003. [CrossRef] [PubMed]
16. Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Stat. 2005;4(4):287–291. [CrossRef]
17. Mikalauskas R, Laurinavicius A. Isometric relaxation combined with active stretching for shoulder pain: a pilot study. J Orthop Sports Phys Ther. 2017;47(12):944–951.
18. Ranzatto ADDS, Chaves TC, Martins MN, Motta DP, Nogueira LC, Meziat-Filho N, et al. Pain intensity scales: a cross-sectional study on the preferences and knowledge of physiotherapists and participants with musculoskeletal pain. Musculoskelet Sci Pract. 2024;73:103162. [CrossRef] [PubMed]
19. Kolber MJ, Fuller C, Marshall J, Wright A, Hanney WJ. The reliability and concurrent validity of scapular plane shoulder elevation measurements using a digital inclinometer and goniometer. Physiother Theory Pract. 2012;28(2):161–168. [CrossRef] [PubMed]
20. Moylan MR, Green TR, Lawton CA. Efficacy of myofascial release in the treatment of myofascial trigger points. J Pain Res. 2013;6:101–108.
21. Lee JH, Kim JH, Lee SW. Myofascial release and active stretching in treating chronic neck pain: a randomized controlled trial. J Musculoskelet Pain. 2018;26(1):67–74.
22. Simons DG, Travell JG. Trigger point release: a systematic review and meta-analysis. Clin J Pain. 2019;35(7):548–554.
23. Mcarthur MP. Myofascial release and its effectiveness in the management of myofascial pain syndrome. J Bodyw Mov Ther. 2015;19(3):512–519.
24. Khan ZK, Ahmed SI, Baig AA, Farooqui WA. Effect of post-isometric relaxation versus myofascial release therapy on pain, functional disability, ROM and QoL in the management of non-specific neck pain: a randomized controlled trial. BMC Musculoskelet Disord. 2022;23(1):567. [CrossRef] [PubMed]
25. Albaker AB. Ischemic pressure vs. post-isometric relaxation for treatment of rhomboid latent myofascial trigger point: a systemic review. Eur Rev Med Pharmacol Sci. 2023;27(11):5031–5038. [CrossRef] [PubMed]
26. Sivalingam AM, Sureshkumar DD, Pandurangan V. Cerebellar pathology in forensic and clinical neuroscience. Ageing Res Rev. 2025;106(102697):102697. [CrossRef] [PubMed]
27. Balaji T, Ramalingam V, Santhana Lakshmi S. Comparing the effects of post-isometric relaxation and hold-relax technique for cervicogenic headache among computer users. Neurol Asia. 2025;30(1):157–163. [CrossRef]
28. Senthilkumar S, Kumar A, Sangeetha S. A study on effectiveness of post isometric relaxation technique in trapezitis among workers. Res J Pharm Technol. 2019;12(10):4836–4840. [CrossRef]
29. Kamalakannan M, Josyula S, Jenifer Augustina A, Naveen M, Hariharan J, Vignesh J, et al. Comparative analysis of high-intensity interval training and traditional rehabilitation programs for accelerated recovery from musculoskeletal injuries. J Back Musculoskelet Rehabil. 2024;37(2):437–443. [CrossRef] [PubMed]
Corresponding author: Sathya Siva, Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai-602105, India. E-mail: sathyasivakannan@gmail.com Tel: +91-9884579620
COPYRIGHT
Published under the CreativeCommonsAttribution-NonCommercial-NoDerivs3.0License.
International Journal of Therapeutic Massage and Bodywork, Volume 19, Number 2, June 2026