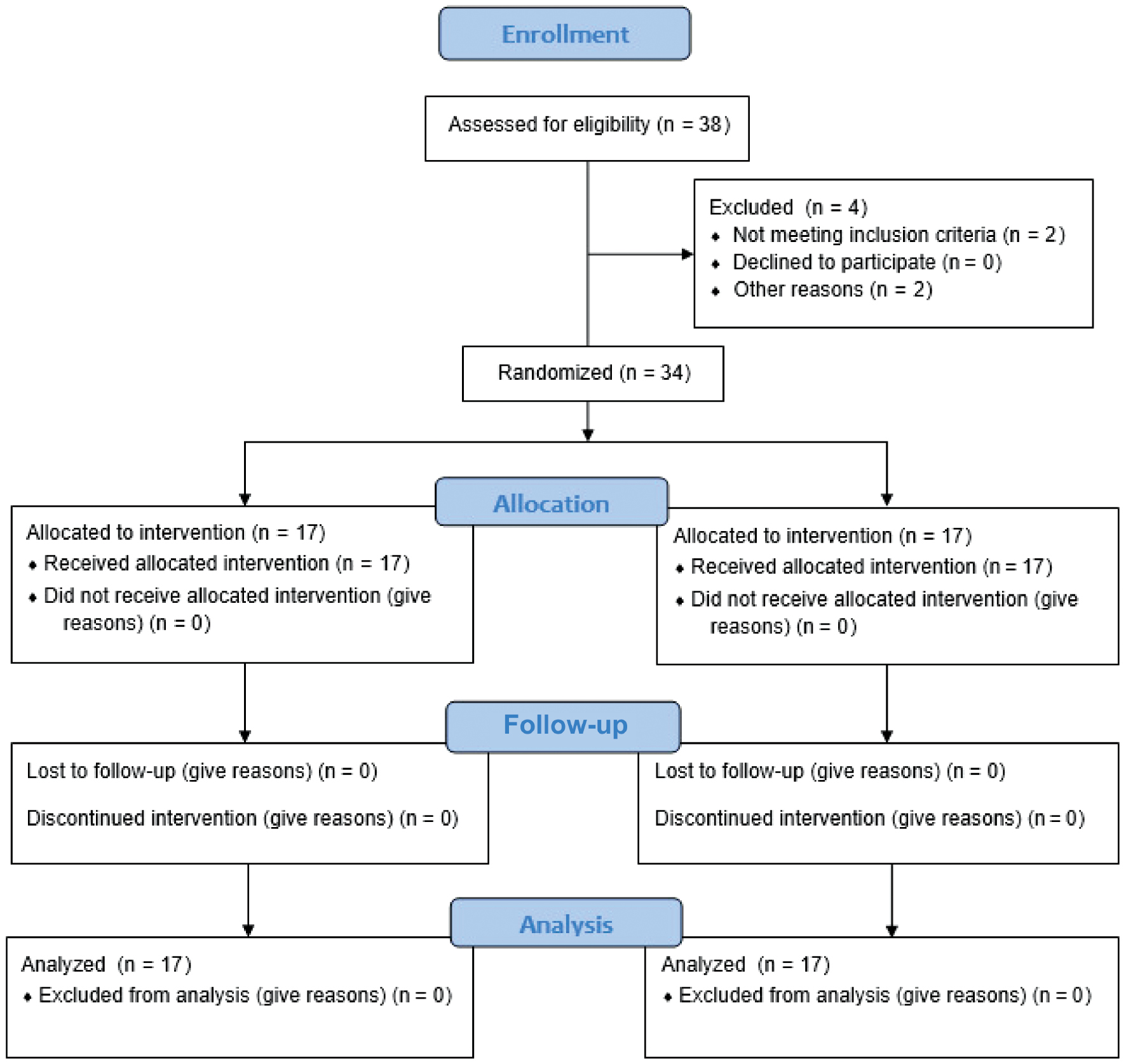
Figure 1. Consolidated Standards of Reporting Trials (CONSORT) flow chart diagram.
| International Journal of Therapeutic Massage and Bodywork (2026) 19(2), 53–63. | https://doi.org/10.3822/ijtmb.v19i2.1279 |
Husin F. Khizar, BPT1, Sathya Siva, MPT1*, Sukumar Ramaswami, MD2, D. Hareeshankar, BPT1, A. Fayaz, BPT1, Prathap Suganthirababu, PhD1
1Department of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India
2Department of Radiology, Saveetha Institute of Medical and Technical Sciences, Chennai, India
Background: Iliotibial band syndrome (ITBS) is a prevalent overuse injury among runners, characterized by lateral knee pain and associated functional limitations. Rehabilitation strategies commonly include manual therapy and strength training, yet their comparative effectiveness remains under investigation. This study aims to evaluate the efficacy of these interventions in reducing pain and promoting functional recovery in runners with ITBS. The findings are intended to inform evidence-based treatment strategies and contribute to the prevention of symptom recurrence.
Methods: Thirty-four runners diagnosed with ITBS were randomly assigned to two equal groups (n = 17). Group A received manual therapy, including deep friction massage, stretching, and soft tissue mobilization. Group B followed a structured strength training program that targeted the hip and knee. The Numerical Pain Rating Scale (NPRS) and Lower Extremity Functional Scale (LEFS) were used to evaluate pain and function, respectively, both before and after a 6-week intervention. Statistical analysis was conducted using the Wilcoxon signed-rank test and the Mann–Whitney U test.
Results: The study indicates that both groups exhibited significant improvements in pain and functional scores following the 6-week intervention. Participants in group A (manual therapy) demonstrated a statistically significant reduction in pain, measured by the NPRS (p = 0.002), and a significant improvement in function, as assessed by the LEFS (p = 0.002). In group B (strength training), there was a statistically significant improvement in both pain, as measured by the NPRS (p < 0.001), and function, as measured by the LEFS (p < 0.001). When comparing post-intervention results between groups, strength training demonstrated greater improvement than manual therapy in both NPRS and LEFS. Future research should consider including a third group that receives a combination of manual therapy and exercise to explore potential synergistic effects.
Conclusion: This pilot study concludes that both manual therapy and strength training are effective in reducing pain and improving function in runners with ITBS. However, strength training demonstrated significantly greater benefits over a 6-week intervention period. These findings support the prioritization of hip- and knee-focused strengthening programs in short-term rehabilitation. Further studies with larger samples and longer follow-up periods are needed, including exploration of combined treatment approaches for potential synergistic health effects.
KEYWORDS: Athletic performance; functional recovery; iliotibial band syndrome; manual therapy; world health organization
Iliotibial band syndrome (ITBS), first described by James Renne in 1975, is a typical overuse injury that results in lateral knee discomfort, particularly among runners and cyclists. It results from irritation or inflammation of the iliotibial band (ITB), a thick fascia that extends from the iliac crest to the proximal tibia, as it repeatedly rubs against the lateral femoral epicondyle.(1) The ITB plays a crucial role in stabilizing the pelvis and knee by transferring forces from the gluteus maximus and tensor fasciae latae to structures like the patella, tibia, and knee joint capsule. It also integrates with muscles such as the biceps femoris and vastus lateralis, facilitating coordination of the lower limb.(2)
A combination of internal and external factors influences the development of ITBS. External factors include high weekly mileage, poor training techniques, frequent hill running, and sudden increases in intensity or distance, as well as uneven or cambered running surfaces, which can increase strain on the ITB. Internal factors include ITB tightness, hip abductor weakness, knee flexor/extensor imbalances, reduced maximum braking power, increased knee flexion during activity and muscular fatigue, inappropriate footwear, and leg length discrepancies. These biomechanical deficits predispose individuals to ITBS by altering lower limb stability and movement patterns.(3)
The hallmark symptom of ITBS is a sharp, burning, or aching lateral knee pain that worsens with repetitive activities like running, especially downhill. In chronic cases, pain persists after exercise and can interfere with walking, stair climbing, or prolonged knee flexion while sitting. Early recognition of symptoms is essential for effective management.(4)
The prevalence of ITBS among runners ranges from 5% to 14%,(5) while general population estimates range from 17% to 48% in women and 45% to 80% in men, reflecting differences in biomechanics and activity levels.(6) Risk factors include a history of lower limb injuries, ITB tightness, improper training practices, inappropriate footwear, uneven running surfaces, leg length discrepancies, and hip or knee muscle weaknesses.(7) Diagnosis relies on clinical tests such as Noble’s compression test, which elicits discomfort over the lateral femoral epicondyle during knee extension(8) and has a reported sensitivity of approximately 30% and specificity of around 88%, and Ober’s test, which assesses ITB tightness. If the patient’s upper leg fails to drop when passively extended and abducted in a side-lying position, ITB tightness is suggested.(9)
Treatment focuses on reducing pain, improving flexibility, and correcting muscle imbalances. Stretching and strengthening exercises targeting the ITB and hip abductors are key to symptom relief. Additional therapies include cortisone injections for acute inflammation, deep transverse friction massage to promote tissue healing, and regular ITB stretching to enhance flexibility. A comprehensive approach combining manual therapy, strength training, and biomechanical corrections is crucial for long-term recovery and injury prevention, particularly in endurance athletes.(10) While previous studies have examined the effects of manual therapy and strength training individually for managing ITBS, few have directly compared these two approaches in a structured clinical trial, particularly in the context of functional recovery and pain reduction in runners. The purpose of this study is to evaluate and compare the efficacy of manual therapy and strength training in a controlled setting, thereby contributing new insights into which intervention may offer superior outcomes for ITBS rehabilitation. This comparative perspective adds value to the existing literature by guiding clinicians in evidence-based decision-making for treating athletic populations.
This pilot study was conducted to explore the feasibility of the research design and procedures. Ethical approval for the study was obtained from the Institutional Scientific Review Board of Saveetha Institute of Medical and Technical Sciences, Chennai, India (ISRB number: 414/07/2024/ISRB/UGSR/SCPT). The study adhered to the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement, which was extended to randomized pilot and feasibility trials (Figure 1).
Figure 1. Consolidated Standards of Reporting Trials (CONSORT) flow chart diagram.
This study was conducted in the Saveetha College of Physiotherapy, Saveetha Hospital, Chennai, India, from the first week of November 2024 to the third week of December 2024. A total of 34 participants were selected using a simple random sampling method from among runners of the sports club at Saveetha Institute who met the inclusion criteria. Participants eligible for the study were those diagnosed with positive Noble’s compression or Ober’s test, active runners (running at least five times per week, both sprint and marathon), aged >18 years, of either gender, and reporting a pain score >5 on the Numerical Pain Rating Scale (NPRS). Exclusion criteria included individuals with previous knee surgeries, other knee pathologies, current use of corticosteroids or pain medications, non-running athletes, pregnancy or breastfeeding, and those with neurological or systemic conditions. After obtaining informed consent, participants were randomly assigned to two groups of 17 using a computer-generated randomization method. Group A, referred to as the manual therapy group, received deep friction massage, gentle stretching, soft tissue mobilization, and foam rolling techniques. Group B, referred to as the strength training group, received a structured exercise regimen including modified side plank, modified side plank with clamshell, side plank with hip abduction, lateral monster walks with TheraBand, single-leg squat, glute bridge with TheraBand, glute bridge with single-leg march, inline lunges, Bulgarian split squat with weights, and double-leg hip thrust. Demographic data were collected from all participants before the intervention(10–12) (Table 1).
Table 1. Demographic Data
| Demographic Data | |
|---|---|
| Gender | |
| Male | 22 |
| Female | 12 |
| Age (years) | |
| 18–24 | 18 |
| 25–30 | 9 |
| 31–35 | 7 |
| Comorbidities | |
| Diabetes mellitus | 2 |
| Hypertension | 10 |
| Thyroid | 0 |
| Body mass index (kg/m2) | |
| 16.5–18.5 (underweight) | 13 |
| 19.5–24.9 (normal weight) | 14 |
| 25–29.9 (overweight) | 7 |
| Number of times involved in running activities per week | |
| 5–7 | 10 |
| 8–9 | 16 |
| ≥10 | 8 |
All subjects were assessed using the NPRS and Lower Extremity Functional Scale (LEFS), both before and after the intervention (first day and after 6 weeks of intervention). The NPRS is a simple and widely used tool to assess pain intensity, where patients rate their pain on a scale from 0 (no pain) to 10 (worst imaginable pain), typically over the past 24 h. Due to its ease of use, it is commonly employed in clinical settings. The minimal clinically important difference (MCID) for the NPRS is 2 points; a change of ≥2 points is considered clinically significant.(13) The LEFS is a 20-item questionnaire used to evaluate functional limitations in individuals with lower limb musculoskeletal disorders. Scores range from 0 to 80, with higher scores indicating better function. LEFS is known for its reliability, validity, and sensitivity to change, with an MCID of 9 points, making it valuable for tracking recovery in conditions like ITBS.(14)
All participants received standardized instructions at the start of the intervention period. They were advised to maintain their usual running routines, provided their pain levels remained tolerable. Participants were instructed to avoid introducing new training variables such as changes in terrain, intensity, or footwear to minimize confounding factors. They were also advised not to take any analgesics or undergo additional treatments during the study period. Adherence to these guidelines was monitored weekly through self-reported activity logs and verbal confirmations.
In the manual therapy group, participants received manual therapy techniques designed to reduce pain and improve soft tissue mobility. The intervention began with a 10- to 15-min deep friction massage, targeting the ITB and adjacent tissues to reduce adhesions, improve circulation, and alleviate localized inflammation (Figure 2). This was followed by gentle stretching exercises—such as the standing ITB stretch and seated figure 4 stretch—performed for 5–10 min to relieve tension and improve flexibility of the ITB and associated structures. Subsequently, soft tissue mobilization was performed using therapist-applied hands-on techniques that involved sustained pressure and slow, controlled strokes directed along the muscle fibers. This technique was applied to the ITB and surrounding muscles, including the tensor fascia latae, gluteal muscles, and quadriceps, for 10–15 min with moderate pressure aimed at reducing myofascial restrictions and muscle tightness (Figure 2). The session concluded with foam rolling applied for 1–2 min and repeated as needed to total 10–15 min, targeting fascial release. Foam rolling of the ITB–tensor fascia latae complex involved positioning the subject’s body parallel to the floor and placing the foam roller between the floor and the thigh, with its long axis perpendicular to the long axis of the thigh. To apply adequate pressure to the area being treated, the subject transferred their body weight to the roller and balanced it with their hands and feet as needed. For the treatment of ITB tissue, the roller was moved from the greater trochanter to the lateral knee joint line. A 2-min rest was provided between each manual technique. This treatment program was administered five times per week over a 6-week period.(10,11)
Figure 2. The sequence of images illustrates various soft tissue mobilization techniques that had been applied to address tightness and dysfunction around the iliotibial band (ITB), tensor fascia latae (TFL), gluteal muscles, and quadriceps. (A) Deep transverse friction massage was performed over the ITB using controlled, perpendicular strokes to reduce adhesions and promote tissue mobility. (B, C) Sustained pressure and slow, targeted mobilization over the TFL and gluteal muscles are demonstrated. These techniques aimed to improve flexibility and reduce myofascial restrictions in the lateral hip region. (D) Deep soft tissue mobilization was directed toward the quadriceps, particularly the distal lateral and medial aspects, to relieve associated tension and improve the overall function of the surrounding musculature. (E) For the ITB tissue release, the foam roller was moved from the greater trochanter to the lateral knee joint line.

Participants in the strength training group followed a structured regimen focusing on strengthening the hip and knee musculature. Strength training has been shown to effectively correct biomechanical deficits and muscle imbalances associated with ITBS, thereby enhancing joint stability, neuromuscular control, and strength in critical muscle groups.(10) These improvements contribute to pain reduction, recurrence prevention, and functional recovery, facilitating a return to pain-free activity with enhanced movement efficiency and reduced risk of injury. The training program was carried out five times per week for 6 weeks with 30-s rest periods between sets and 1-min rest intervals between different exercises in the clinical step-up at Saveetha Sports Club. The weekly exercise progression is detailed in Table 2.
Table 2. Six-week Progressive Strengthening Protocol for ITBS Rehabilitation
| Exercise | Week | Sets | Reps | Hold | Primary Muscles Targeted |
|---|---|---|---|---|---|
| Modified side plank | Week 1 | 2 | 15 | 5 s | Core, gluteus medius, obliques |
| Week 2 | 3 | 20–25 | 5 s | ||
| Modified side plank with clamshell | Week 1 | 2 | 15 | 5 s | Gluteus medius, external rotators, core |
| Week 2 | 3 | 15–20 | 5 s | ||
| Side plank with hip abduction | Week 1 | 2 | 15 | 5 s | Gluteus medius/minimus, core |
| Week 2 | 3 | 20 | 5 s | ||
| Lateral monster walk with TheraBand | Week 1 | 2 | 15 | — | Gluteus medius, tensor fasciae latae |
| Week 2 | 3 | 20–25 | — | ||
| Week 3 | 3 | 25–30 | — | ||
| Single-leg squat | Week 2 | 2 | 12–15 | 2 s | Quadriceps, gluteus maximus, core |
| Week 3 | 2 | 15–20 | 2 s | ||
| Week 4 | 3 | 25 | 2 s | ||
| Glute bridge with TheraBand | Week 2 | 2 | 15 | 5 s | Gluteus maximus, hamstrings, core |
| Week 3 | 3 | 15–20 | 5 s | ||
| Week 4 | 3 | 20–25 | 5 s | ||
| Week 5 | 3 | 25–30 | 5 s | ||
| Glute bridge with single-leg march | Week 2 | 2 | 15 | 5 s | Gluteus maximus, core, hip flexors (stabilizing) |
| Week 3 | 3 | 15–20 | 5 s | ||
| Week 4 | 3 | 20–25 | 5 s | ||
| Week 5 | 3 | 25–30 | 5 s | ||
| Inline lunges | Week 5 | 3 | 20 | — | Gluteus maximus, quadriceps, hamstrings |
| Week 6 | 3 | 25–30 | — | ||
| Bulgarian split squat with weights | Week 5 | 2 | 12–15 | — | Gluteus maximus, hamstrings, core |
| Week 6 | 3 | 15–20 | — | ||
| Double-leg hip thrust | Week 5 | 2 | 12–15 | — | Gluteus maximus, hamstrings |
| Week 6 | 3 | 15–20 | — |
Exercises focus on progressive overload to improve strength, stability, and neuromuscular control. Primary muscle groups targeted are listed to illustrate therapeutic intent. Progression in sets, repetitions, and complexity was based on the principles of progressive overload and neuromuscular adaptation, aiming to build hip stability, improve movement control, and address biomechanical deficits associated with ITBS.
ITBS = iliotibial band syndrome.
All data were analyzed using SPSS version 27 was developed and distributed by IBM Corp. (Armonk, New York, USA). Descriptive statistics, including percentages, were used to summarize the demographic variables such as age and sex. For inferential analysis, the Shapiro–Wilk test was conducted to assess the normality of the data. Since the data were not normally distributed, non-parametric tests were employed. The Wilcoxon signed-rank test was used to assess within-group differences in NPRS and LEFS scores for groups A and B. The Mann–Whitney U test was applied to compare differences between the two groups. These non-parametric tests are suitable for small sample sizes and data that are not normally distributed. Demographic characteristics (age and sex) are presented in Table 3. Within-group differences in NPRS and LEFS scores are shown in Table 4, while Table 5 presents the between-group comparisons.
Table 3. Age and Sex Distribution of Samples
| Age (years) | Group A | Group B | ||||
|---|---|---|---|---|---|---|
| Male | Female | Total | Male | Female | Total | |
| 18–24 | 8 | 2 | 10 | 6 | 2 | 8 |
| 25–30 | 2 | 2 | 4 | 3 | 2 | 5 |
| 31–35 | 1 | 2 | 3 | 2 | 2 | 4 |
| Total | 11 | 6 | 17 | 11 | 6 | 17 |
Table 4. Within-group Comparison of NPRS and LEFS Scores in Group A and Group B (Pre-test vs. Post-test)
| Pre-test Mean ± SD | Post-test Mean ± SD | Z Value | p-value | |
|---|---|---|---|---|
| Outcome NPRS | ||||
| Group A (n = 17) | 8.88 ± 0.928 | 8.12 ± 0.928 | −3.127 | 0.002 |
| Group B (n = 17) | 8.41 ± 1.064 | 2.88 ± 0.781 | −3.727 | <0.001 |
| Outcome LEFS | ||||
| Group A (n = 17) | 43.94 ± 12.26 | 50.24 ± 10.341 | −3.068 | 0.002 |
| Group B (n = 17) | 41.12 ± 11.768 | 57.33 ± 10.229 | −3.625 | <0.001 |
LEFS = Lower Extremity Functional Scale; NPRS = Numerical Pain Rating Scale.
Table 5. Between-group Comparison of NPRS and LEFS Scores Between Group A and Group B
| Mean ± SD | Z Value | W | U | p-value | r Value | |
|---|---|---|---|---|---|---|
| Outcome NPRS | ||||||
| Pre-test | 7.91 ± 1.138 | −2.051 | 240.00 | 87.00 | 0.040 | 0.351 |
| Post-test | 4.35 ± 2.087 | −4.870 | 159.00 | 6.00 | <0.001 | 0.835 |
| Outcome LEFS | ||||||
| Pre-test | 42.53 ± 11.920 | −0.707 | 277.00 | 124.00 | 0.480 | 0.121 |
| Post-test | 53.88 ± 10.784 | −2.158 | 235.00 | 82.00 | 0.031 | 0.370 |
LEFS = Lower Extremity Functional Scale; NPRS = Numerical Pain Rating Scale; SD = standard deviation.
The study found that among the 17 patients in group A, 10 (59%) were aged 18–24 years, 4 (23%) were aged 25–30 years, and 3 (18%) were aged 31–35 years. In contrast, in group B, 8 (47%) were aged 18–24 years, 5 (29%) were aged 25–30 years, and only 4 (24%) were aged 31–35 years (Table 3).
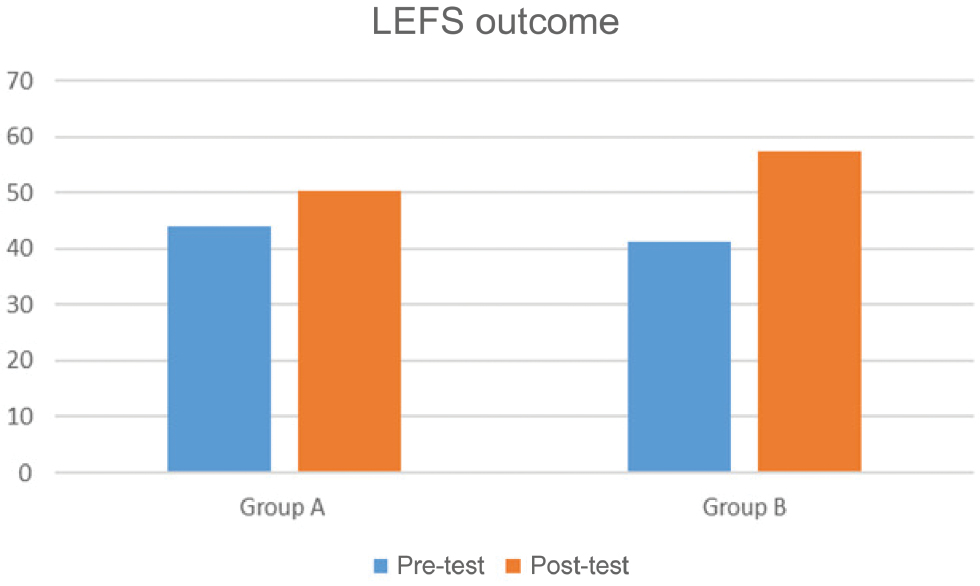
A Wilcoxon signed-rank test revealed statistically significant improvements in pain scores (NPRS) after the 6-week intervention in both groups. For group B, the test yielded Z = −3.727, p ≤ 0.001, while for group A, the test yielded Z = −3.127, p = 0.002 (Table 4, Figure 3). Functional scores (LEFS) also showed significant improvement, with group B yielding Z = −3.625, p < 0.001 and group A yielding Z = −3.068, p = 0.002 (Table 4, Figure 4).
Figure 3. Graphical representation of NPRS outcome for pre- and post-test. NPRS = Numerical Pain Rating Scale.
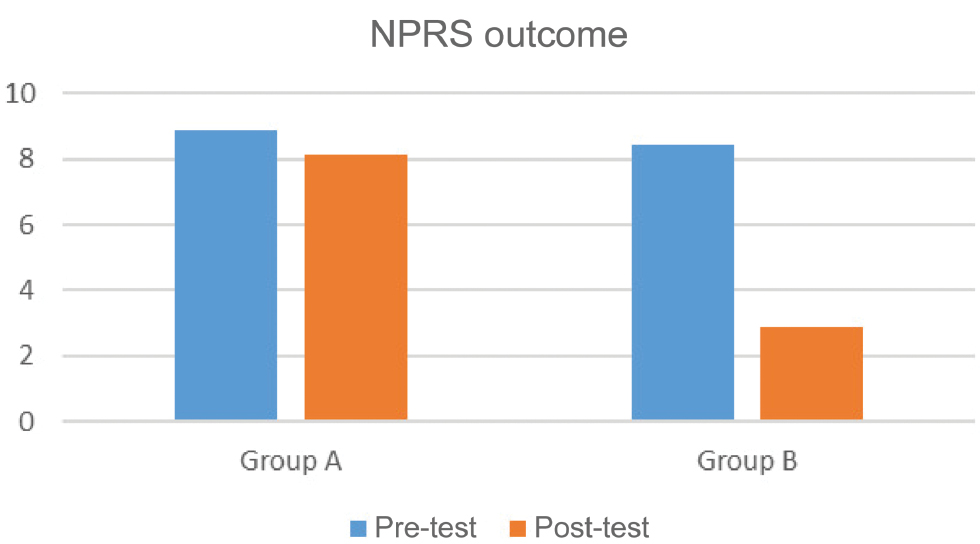
Figure 4. Graphical representation of LEFS outcome for pre- and post-test. LEFS = Lower Extremity Functional Scale.
The Mann–Whitney U test indicated a statistically significant difference in post-intervention NPRS scores between group A and group B (U = 6.00, p < 0.001). As the p-value was less than the alpha level of 0.05, the null hypothesis was rejected, suggesting that the treatment method had a significant effect on pain reduction in ITBS. The effect size (r) for the pre-test was approximately 0.351, indicating a small effect, while the post-test r value was approximately 0.835, indicating a large effect (Table 5). For LEFS, a significant difference was also observed in the post-test comparison between the two groups (U = 82.00, p = 0.031). Again, the p-value was below the 0.05 threshold, leading to rejection of the null hypothesis. The pre-test r value was approximately 0.121, indicating a small effect size, whereas the post-test r value was approximately 0.370, indicating a medium effect size (Table 5).
This pilot study reinforces the growing consensus that strength training is a fundamental component of ITBS rehabilitation, offering a more sustainable approach to both recovery and injury prevention in runners. ITBS is one of the most common causes of knee pain among female runners, as demonstrated in a study by Ferber et al.(15)
According to the study by Christofi et al., manual therapy, stretching, strengthening exercises, neurological and muscular re-education, and biomechanical adjustments are all frequently used physiotherapy treatments. Because strengthening exercises can help with muscular imbalances associated with ITBS, they were commonly used, especially for the hip abductors and external rotators. Additionally, stretching and manual therapy were used to increase tissue mobility and lessen pain. However, direct comparisons are limited by the variations in treatments and outcome measures among researchers. Although there is some evidence that multimodal physiotherapy can effectively reduce pain and improve function, more studies are necessary because there are not many high-quality randomized controlled trials.(16) The recognition of strength training as a crucial intervention for ITBS is growing, particularly in addressing muscle imbalances and mobility deficits. Several studies have linked deficits in hip and knee strength, especially in the hip abductors and external rotators, to the development of ITBS. Individuals with ITBS often exhibit hip abductor weakness, which leads to excessive internal rotation of the hip and increased knee adduction during running. These biomechanical alterations contribute to excessive strain on the ITB, exacerbating the pain and dysfunction described by Fredericson and Weir(17). Ferber et al.’s research demonstrated that targeted strengthening of these muscle groups plays a key role in alleviating symptoms and correcting faulty movement patterns. Strength training programs focused on the hip abductors and external rotators have been shown to improve neuromuscular control, reduce aberrant kinematics, and enhance overall functional performance. By increasing hip stability and reducing excessive movement at the knee, strength training helps to address the underlying causes of ITBS rather than just managing symptoms. Incorporating progressive strength training into treatment protocols can lead to more effective and long-term recovery for runners affected by ITBS.(18)
According to a study by Willy et al., targeted strength training plays a crucial role in improving running mechanics and neuromuscular control, ultimately helping to prevent the recurrence of ITBS. Strengthening exercises that focused on the hip abductors and external rotators have been shown to correct biomechanical deficits, reducing excessive hip internal rotation and knee adduction—two common movement patterns associated with ITBS. By addressing these underlying issues, strength training not only aids in symptom relief but also enhances overall running efficiency.(19) Further evidence supporting the effectiveness of strength training comes from Dolak et al., who found that a structured 6-week hip strengthening program led to significant improvements in running kinematics and a notable reduction in ITBS symptoms. These findings align with our study’s findings, which demonstrated that strength training produced greater pain reduction and functional improvements compared to manual therapy. While manual therapy may provide temporary symptom relief, it does not directly influence neuromuscular adaptations or long-term biomechanical corrections.(20)
In addition to the strengthening exercises discussed, emerging evidence supports the incorporation of soft tissue techniques as a complementary intervention for managing ITBS. Manual therapy techniques, such as myofascial release, deep tissue massage, and soft tissue mobilization, are commonly used to alleviate ITB tightness and soreness, as noted in a study by Fredericson and Weir(17). While these methods may offer short-term symptom relief, their effectiveness as stand-alone treatments remains uncertain.(17) These treatments may help manage symptoms in the short term, but they do not correct underlying muscular imbalances and movement dysfunctions that contribute to ITBS, making long-term recovery challenging.(21–26) Although manual therapy may offer temporary relief, strength training addresses the underlying biomechanical deficiencies that contribute to ITBS, resulting in more substantial and long-lasting benefits. Given the growing body of research supporting strength-based rehabilitation, specific strengthening interventions may be considered a priority in the management of runners recovering from ITBS.
Additional studies further support their short-term benefits. Beers et al. demonstrated that instrument-assisted soft tissue mobilization can improve flexibility and reduce discomfort in athletes with ITB tightness.(27) Similarly, Mohr et al. found that foam rolling and other self-myofascial release techniques can significantly reduce ITB-related pain and improve tissue mobility in the short term.(28)
Several studies have investigated the combined effects of soft tissue techniques and exercise in ITBS management. For instance, a study by Schwellnus et al. combined stretching, deep tissue massage, and strengthening exercises in endurance runners with ITBS, showing more consistent pain reduction and faster return to sport compared to exercise alone.(29) While more high-quality trials are needed, these findings suggest that integrating soft tissue therapy with a structured exercise program may offer additive or synergistic benefits.
Limitations of our study include the small sample size, which restricts the broad applicability of the results to a larger group of runners. The study duration may not be sufficient to assess the long-term effects of manual therapy and strength training. Variability in participants’ adherence to the intervention protocol could affect the outcomes. Additionally, factors such as running biomechanics, footwear, and training intensity were not strictly controlled, which may have influenced the results. Larger sample sizes, longer follow-up times, and objective biomechanical analysis are suggested for future studies.
This pilot study concludes that both manual therapy and strength training are effective in reducing pain and improving functional outcomes in runners diagnosed with ITBS. However, strength training resulted in significantly greater improvements in both pain reduction and functional recovery over a 6-week period. These findings suggest that strengthening interventions targeting the hip and knee musculature may be more beneficial than manual therapy alone in the short-term rehabilitation of ITBS in runners. Based on these results, health-care professionals managing ITBS in runners may consider incorporating hip- and knee-focused strength training programs to enhance recovery outcomes related to pain and function. This evidence may inform treatment planning, where time efficiency and functional improvements are critical considerations. Nonetheless, further research with larger sample sizes and extended follow-up periods is necessary. Future studies should also include objective biomechanical assessments (e.g., gait analysis, muscle strength testing, range-of-motion measurements) to complement self-reported outcomes and provide a more comprehensive evaluation of treatment efficacy. Future research should also consider including a third group that receives a combination of manual therapy and exercise to investigate potential synergistic effects. Additionally, exploring the effects of combined manual therapy and exercise interventions could help determine whether a multimodal approach offers synergistic benefits.
The authors declare there are no conflicts of interest.
No sources of funding were used in this study.
Study design/planning: Husin F. Khizar, Sathya Siva, and Prathap Suganthirababu. Data collection/entry and literature analysis/search: D. Hareeshankar and A. Fayaz. Data analysis: Sukumar Ramaswami and Sathya Siva. Statistics and interpretation: Sathya Siva. Preparation of the manuscript: Husin F. Khizar and Sathya Siva.
1. Ellis R, Hing W, Reid D. Iliotibial band friction syndrome – A systematic review. Man Ther. 2007;12:200–208. [CrossRef] [PubMed]
2. Friede MC, Innerhofer G, Fink C, Alegre LM, Csapo R. Conservative treatment of iliotibial band syndrome in runners: Are we targeting the right goals? Phys Ther Sport. 2022;54:44–52. [CrossRef] [PubMed]
3. Weckström K, Söderström J. Radial extracorporeal shockwave therapy compared with manual therapy in runners with iliotibial band syndrome. J Back Musculoskelet Rehabil. 2016;29(1):161–170. [CrossRef] [PubMed]
4. Kirk KL, Kuklo T, Klemme W. Iliotibial band friction syndrome. Orthopedics. 2000;23(11):1209–1214; discussion 1214–1215; quiz 1216–1217. [CrossRef] [PubMed]
5. van der Worp MP, van der Horst N, de Wijer A, Backx FJ, Nijhuis-van der Sanden MW. Iliotibial band syndrome in runners: A systematic review. Sports Med. 2012;42:969–992. [CrossRef] [PubMed]
6. Buist I, Bredeweg SW, Lemmink KAPM, van Mechelen W, Diercks RL. Predictors of running-related injuries in novice runners enrolled in a systematic training program: A prospective cohort study. Am J Sports Med. 2010;38(2):273–280. [CrossRef] [PubMed]
7. McKay J, Maffulli N, Aicale R, Taunton J. Iliotibial band syndrome rehabilitation in female runners: A pilot randomized study. J Orthop Surg Res. 2020;15(1):188. [CrossRef] [PubMed]
8. Sandeep R, Saha J, Mishra L, Bhowmik S. Development and content validation of Iliotibial Band Friction Syndrome index (IBFS-I). J Clin Diagn Res. 2024;18:9. [CrossRef]
9. Sanchez-Alvarado A, Bokil C, Cassel M, Engel T. Effects of conservative treatment strategies for iliotibial band syndrome on pain and function in runners: A systematic review. Front Sports Act Living. 2024;6:1386456. [CrossRef] [PubMed]
10. Shamus J, Shamus E. The management of iliotibial band syndrome with a multifaceted approach: A double case report. Int J Sports Phys Ther. 2015;10(3):378–390. [PubMed]
11. Opara M, Kozinc Ž. Stretching and releasing of iliotibial band complex in patients with iliotibial band syndrome: A narrative review. J Funct Morphol Kinesiol. 2023;8(2):74. [CrossRef] [PubMed]
12. Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 2000;10(3):169–175. [CrossRef] [PubMed]
13. Boonstra AM, Schiphorst Preuper HR, Balk GA, Stewart RE. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain. 2014;155(12):2545–2550. [CrossRef] [PubMed]
14. Mehta SP, Fulton A, Quach C, Thistle M, Toledo C, Evans NA. Measurement properties of the Lower Extremity Functional Scale: A systematic review. J Orthop Sports Phys Ther. 2016;46(3):200–216. [CrossRef] [PubMed]
15. Ferber R, Noehren B, Hamill J, Davis I. Competitive female runners with a history of iliotibial band syndrome demonstrate atypical hip and knee kinematics. J Orthop Sports Phys Ther. 2010;40(2):52–58. [CrossRef] [PubMed]
16. Christofi I, Ploutarchou G, Savva C, Karagiannis C. The effectiveness and characteristics of physiotherapy interventions on adults with iliotibial band syndrome. A systematic scoping review. J Bodyw Mov Ther. 2024;40:1939–1948. [CrossRef] [PubMed]
17. Fredericson M, Weir A. Practical management of iliotibial band friction syndrome in runners. Clin J Sport Med. 2006;16(3):261–268. [CrossRef] [PubMed]
18. Ferber R, Kendall KD, Farr L. Changes in knee biomechanics after a hip-abductor strengthening protocol for runners with patellofemoral pain syndrome. J Athl Train. 2011;46(2):142–149. [CrossRef] [PubMed]
19. Willy RW, Davis IS. The effect of a hip-strengthening program on mechanics during running and during a single-leg squat. J Orthop Sports Phys Ther. 2011;41(9):625–632. [CrossRef] [PubMed]
20. Dolak KL, Silkman C, Mckeon M, Hosey JM, Kerrigan RG. Hip strengthening to improve running mechanics and treat iliotibial band syndrome. J Athl Train. 2011;46(2):196–202.
21. Sivanandam M, Jothilingam M, Purushothaman S. Integrated neuromuscular inhibition technique for myofascial trigger point pain relief: A systematic review. Fiz Pol. 2024;24(5):162–165. [CrossRef]
22. Al-Mhanna SB, Batrakoulis A, Norhayati MN, Mohamed M, Drenowatz C, Irekeola AA, et al. Combined aerobic and resistance training improves body composition, alters cardiometabolic risk, and ameliorates cancer-related indicators in breast cancer patients and survivors with overweight/obesity: A systematic review and meta-analysis of randomized controlled trials. J Sports Sci Med. 2024;23(2):366–395. [CrossRef] [PubMed]
23. Kamalakannan M, Josyula S, Jenifer Augustina S, Naveen M, Hariharan J, Vignesh J, et al. Comparative analysis of high-intensity interval training and traditional rehabilitation programs for accelerated recovery from musculoskeletal injuries. J Back Musculoskelet Rehabil. 2024;37(2):437–443. [CrossRef] [PubMed]
24. Kotteeswaran K, Shanmugasundaram N, Shalini S, Sowmya MV. Effect of multidirectional and unidirectional wobble board lateral step-up exercise in pain, symptom and ADL among unilateral medial compartmental osteoarthrosis of knee. Biomedicine. 2021;41(3):669–677. [CrossRef]
25. Masi AT, Nair K, Evans T, Ghandour Y. Clinical, biomechanical, and physiological translational interpretations of human resting myofascial tone or tension. Int J Ther Massage Bodywork. 2010;3(4):16–28. [CrossRef] [PubMed]
26. Balaji T, Ramalingam V, Santhana Lakshmi S. Comparing the effects of post-isometric relaxation and hold-relax technique for cervicogenic headache among computer users. Neurol Asia. 2025;30(1):157–163. [CrossRef]
27. Beers A, Ryan M, Kasimer M, Macintyre D, Taunton J. The effectiveness of instrument-assisted soft tissue mobilization for iliotibial band syndrome. J Orthop Sports Phys Ther. 2008;38(9):591–597.
28. Mohr AR, Long BC, Goad CL. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J Sport Rehabil. 2014;23(4):296–299. [CrossRef] [PubMed]
29. Schwellnus MP, Derman EW, Noakes TD. Aetiology of skeletal muscle “cramps” during exercise: A novel hypothesis. J Sports Sci. 1997;15(3):277–285. [CrossRef] [PubMed]
Corresponding author: Sathya Siva, Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India. E-mail: sathyasivakannan@gmail.com Tel: +9884579620
COPYRIGHT
Published under the CreativeCommonsAttribution-NonCommercial-NoDerivs 3.0 License.
International Journal of Therapeutic Massage and Bodywork, Volume 19, Number 2, June 2026