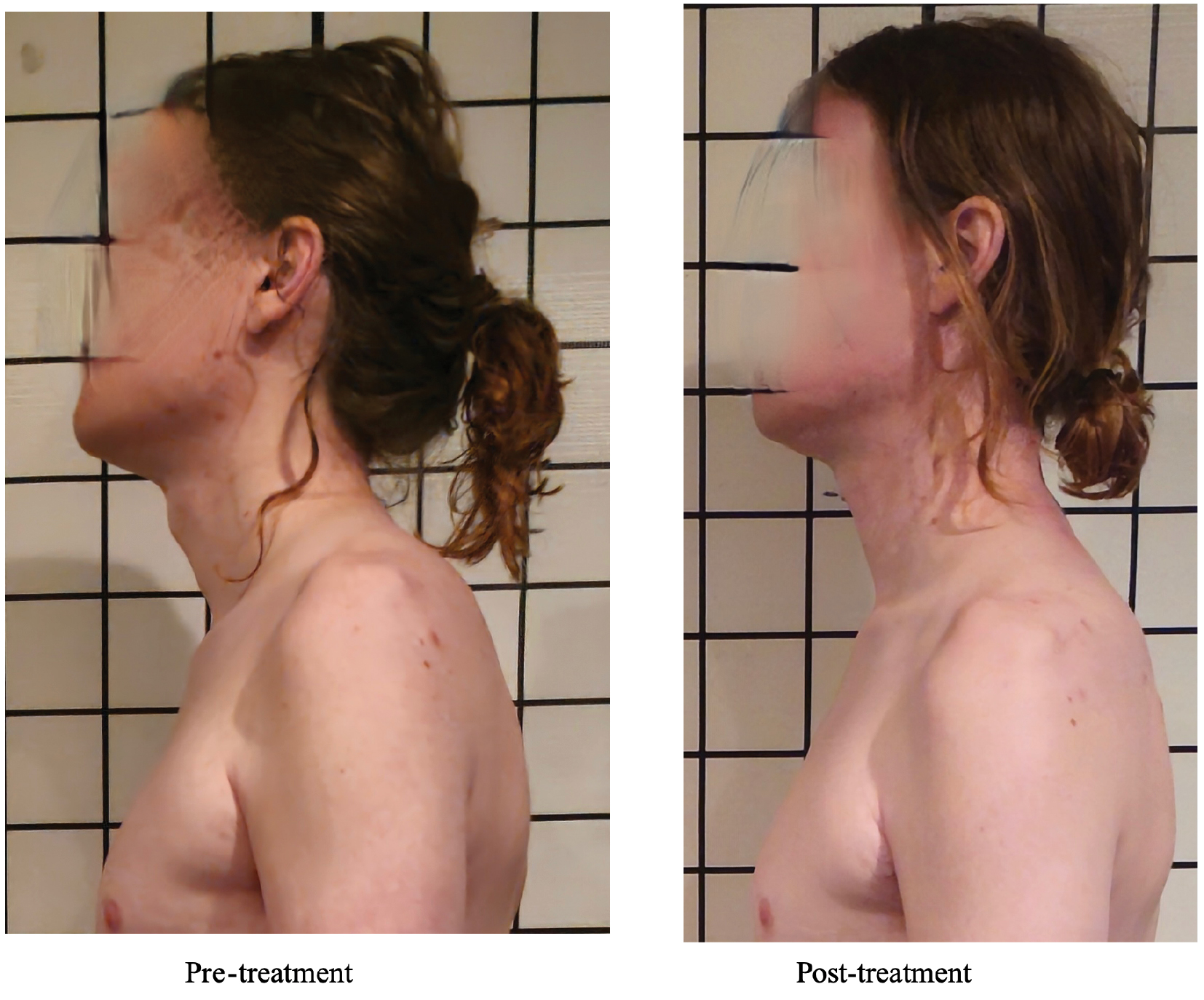
Figure 1. Posture pre–post treatment (face blurred for privacy).
| International Journal of Therapeutic Massage and Bodywork (2026) 19(2), 27–45. | https://doi.org/10.3822/ijtmb.v19i2.1215 |
Ralph Magliano, MA, CCC-SLP, LMT1*
1School of Health Sciences, Harrisburg Area Community College, Harrisburg, PA, USA
Introduction: Behavioral dysphonia is a voice condition in which inefficient muscle tension and misuse interrupt the ability of the body to produce the desired vocal function and quality. Treatment methods typically incorporate traditional voice therapy with manual laryngeal manipulation. A lack of treatment approaches for dysphonia exists that address the vocal system including all its subsystems (i.e., breath, phonation, resonance, articulation) and posture. A limited number of reports exist describing the effect of massage therapy to address the vocal system anatomy of a singer with behavioral dysphonia.
Objective: This case report explores the effects of a massage protocol targeting the vocal system of a person with symptoms of behavioral dysphonia when singing.
Case presentation: A massage student completing an 8-month massage therapy program performed 90-min massage sessions twice a week for 3 weeks on a 33-year-old student singer/songwriter referred by his vocal instructor with symptoms of behavioral dysphonia. Symptoms presented only during singing and included “tensing up,” effortful voice, and vocal fatigue. Massage therapy sessions targeted the structure, musculature, and connective tissue of the whole vocal anatomy. Acoustic, aerodynamic, and physical outcomes were measured pre and post treatment.
Results: Baseline forward head posture, elevated shoulder position, cervical hyperlordosis, and thoracic hyperkyphosis, as well as thoracic/head/neck engagement during singing all decreased. Low laryngeal posture neutralized. Vocal range increased by six whole tones. Despite between-session variability, following the final session, loudness had increased by 6 dB, peak expiratory flow by 174 L/min, and inspiratory abdominal wall movement by 5 cm. Maximum phonation time improved within all sessions except on the final day. Functional measures for respiratory fluency, harmonics-to-noise ratio, and vocal range during singing all improved. Singing Voice Handicap Index improved by 9 points but remained below norms.
Discussion: A massage protocol addressing the whole vocal anatomy produced positive aerodynamic, acoustic, and physical outcomes in a person who presented with behavioral dysphonia when singing.
KEYWORDS: Massage; voice; singing; tension; dysphonia
Dysphonia is a deviation from one’s normal or desired vocal quality and function, resulting in voice produced with some degree of difficulty, inefficiency, or compromised stability. When dysphonia is related to inappropriate vocal behavior (e.g., poor technique, excess muscle tension, vocal misuse, or abuse), it is referred to as behavioral dysphonia.(1) Behavioral dysphonia can interfere with function, balance, or coordination at or between any level of respiration, phonation, resonance, or articulation.(2–4) These subsystems of vocal function and their respective anatomy are hereby referred to collectively as “the vocal system.”
Behavioral dysphonia has been associated with excess muscle tension activated in the laryngeal and supra/infrahyoid components of the vocal system anatomy.(1,2,4–8) Research also acknowledges the involvement of the anterior neck, cervical vertebrae, scapulae, and muscles of the thoracic cage.(1,2,9–11) Clinical manifestations may include elevated larynx, forward head posture, decreased jaw range of motion (ROM), hypertonic neck muscles, elevated shoulders, exaggerated cervical lordosis or thoracic kyphosis, a thoracic breathing pattern, and poor breath control.(9,10,12–15) Vocal symptoms can include unstable, strained, effortful, breathy, or hoarse voice quality, as well as limited vocal range, decreased loudness, and vocal fatigue.(1–3,16,17)
Underlying etiologies are not fully understood. Studies have attributed symptoms to sympathetic nervous system activation,(18) posture,(10–14) high vocal demand, personality, and even psychological factors including stress and low confidence.(17,19–21)
Typically, dysphonia is treated by speech pathologists using exercises and coaching to improve vocal efficiency.(2,22,23) Increasingly, the literature is exploring the benefit of manual techniques.(24) Much of the literature investigates variations on a technique first described by Aronson in 1990 as “manual circumlaryngeal therapy” (MCT).(3) MCT addresses restrictive tension elevating the larynx with massage and manipulation of the larynx, thyrohyoid space, hyoid bone, and suprahyoid musculature while the patient hums or sustains a vowel.(3,5–7) Positive changes are then reinforced with voice therapy. In 2009, a variation of MCT called laryngeal manual therapy (LMT) was introduced by Mathieson et al.(25) LMT incorporates manipulation of the larynx and hyoid with massage of the sternocleidomastoid muscles and “kneading” of the supralaryngeal area.(25,26) MCT and LMT have both demonstrated improvements in vocal quality.(1,7,8,25–27) While MCT and LMT address restrictive tension in the laryngeal and perilaryngeal areas, other studies consider muscles of the face,(1) tongue, head, neck,(28) and those involved in breath and posture.(28,29)
Three published studies have investigated a massage protocol for the voice created by a professional massage therapist.(30–32) This method, developed by Leena Koskinen in cooperation with physicians and voice professionals, is called “voice massage” (VM). While a key intention of soft-tissue intervention is the release of tissue hypertonicity, the goal of VM is instead “active relaxation” with an aim to “improve subjects’ awareness of the state of the muscles and the processes of breathing, phonation, and articulation.” “The muscles are not massaged to the point of becoming flabby.”(30) VM uses professional massage strokes to address the vocal system, targeting postural muscles and musculature affecting resonance, phonation, and articulation. VM does not directly address the larynx or the diaphragm with massage, but addresses their function with humming, phonation, stretching, and exercises. VM studies have shown mixed results and have all involved non-singing healthy subjects.
The massage protocol reported here differs from VM in philosophy in that a key therapeutic goal of this protocol is intentional release of tissue hypertonicity.(33) Also, unlike VM and MCT, this protocol did not include vocal exercises, in order to isolate the effects of massage alone. Like VM, this massage protocol’s focus was vocal anatomy outside the larynx but also expanded its scope to address deep and interconnected muscles of the vocal system including the tongue and primary and secondary muscles of respiration. Direct laryngeal manipulation was excluded, as it was hypothesized that although the larynx would receive only incidental contact (i.e., a superficial connective tissue stroke over the sternohyoid region), the client’s vocal symptoms might improve due to the integrative nature of voice production as a whole-body phenomenon. Although a case report cannot establish causation, the guiding question of this study was: “Can a whole-body massage protocol targeting hypertonicity in the vocal system without a direct focus on the larynx and without inclusion of vocal training improve vocal function in a person presenting with symptoms of behavioral dysphonia when singing?”
A 33-year-old male student singer/songwriter, with no diagnosed vocal pathology, was referred to Harrisburg Area Community College (HACC) massage clinic by his vocal instructor. The client had received formal vocal instruction from this instructor for two semesters (i.e., 30 1-h lessons). The instructor reported that, when singing, the client complained of throat tightness, had poor respiratory control, “tightened and squeezed” his throat, and sometimes “barely opened his mouth.” These habits “held back the free flow” of his singing voice and affected his breath, loudness, sound quality, and ability to sustain notes, occasionally leading to vocal fatigue and hoarseness by the end of their lessons. The client and his instructor reported that his speaking voice was normal and without symptom or complaint. The client first noticed vocal difficulty 5 years earlier when teaching himself to sing, and his two semesters of voice lessons were the only intervention. His medical history was unremarkable except that he had been prescribed Sublocade, a slow-release subcutaneous injection in the abdominal area. He reported this medication had not affected his voice, and he was cleared by his physician for massage as long as a general precaution was implemented over the area. While undergoing massage treatment, the client received no other therapies or intervention.
During the initial interview, the client expressed that he associated singing with fear and described a growing anxiety and a persistent “tensing up” when singing that he felt in his breath, posture, and voice, especially when attempting to sing loudly.
Standard vocal assessment can include physical, acoustic, aerodynamic, and self-assessment measures. This study incorporated a comprehensive battery of these measures to capture a broad and dynamic image of treatment effects on both the structure of the vocal system (i.e., posture, mandibular ROM, abdominal movement),(9,10,12–15) its function as it relates to the client’s dysphonia (i.e., harmonics-to-noise ratio (HNR), jitter, shimmer, maximum phonation time (MPT), loudness, vocal range, peak expiratory flow (PEF), breath fluency), and its impact on the client (i.e., Singing Voice Handicap Index (S-VHI) and a client journal).(2,3,16–21,34–43) All data, except client self-assessment, were collected by the therapist who was also the sole evaluator. All assessment procedures and outcomes used in the study were supported by the literature(18–20,34–43) and explained to the client before data collection. Table 1 provides a visual summary of assessment measures.
Table 1. Visual Summary of Assessment Measures
| Category | Outcome Measure | Purpose |
|---|---|---|
| Physical | Posture Mandibular range of motion (ROM) Dynamic breath assessment |
To assess structure and movement affecting articulation, resonance, and breath |
| Acoustic | Jitter (loudness instability), shimmer (pitch instability), harmonics-to-noise ratio (HNR; amount of turbulent noise vs. harmonic resonance), vocal range (range of pitches produced efficiently) | To measure voice quality and flexibility |
| Aerodynamic | Maximum phonation time (MPT), peak expiratory flow (PEF) | To measure respiratory strength, endurance, and coordination |
| Subjective | Singing Voice Handicap Index (S-VHI) | A self-assessment of the perceived personal impact of vocal condition |
| Functional | Functional vocal range Functional HNR Breath fluency |
To assess vocal range, turbulence in pure vocal vibration, and breath coordination during actual singing |
Visual posture/breath assessment
Posture: The influence of posture on voice is well documented.(10–14,34) Upon visual assessment, the client presented with forward head posture, slight cervical hyperlordosis, slightly forward and elevated shoulders, and downward rotation of scapulae with the left acromion process elevated higher than the right. Hip position appeared symmetrical and balanced with no overt anterior/posterior tilt, so lower body was not explicitly targeted in this case.
Mandibular range of motion (ROM): Limited mandibular ROM is associated with behavioral dysphonia.(6,13,15) The student was instructed to produce the open vowel /a/, and a measurement was taken from his upper to lower incisors.
Breath: Upon instruction to “take a comfortable deep breath,” the client demonstrated neck extension, shoulder elevation, and thoracic expansion, appearing to engage accessory muscles to increase lung capacity. These symptoms were not present during tidal breath.
Inspiratory abdominal wall movement: This outcome is associated with laryngeal tension and breath support.(9,44) A flexible tape measure was placed around the subject’s abdominal wall, at the level of the navel. He was instructed to “take a full range of motion breath letting his abdominal muscles fully relax.” A measurement was taken at maximum inhalation.
Acoustic outcome measures
For all acoustic measures, the client was instructed to stand comfortably with his hands at his sides. Acoustic measures were recorded in a quiet room (<40 dB) with the client’s mouth approximately 15 cm from a stand-mounted microphone chosen for its wide frequency range, relatively flat frequency response, and low self-noise, consistent with recommended standards for accurate data collection of voice.(45) Data were saved in 24-bit digital format and acquired by a sampling frequency of 96,000 Hz to maximize sample quality. Data were later analyzed by the Voce-Vista (Voice Science Works, Montclair, NJ, USA) and Praat (Paul Boersma and David Weenink, University of Amsterdam; Amsterdam, Netherlands)(46) speech analysis software. All acoustic voice data collection procedures followed researched standards for maximum data accuracy(37,38,45) and were consistent from session to session.
Voice quality—jitter, shimmer, and HNR: Voice quality was assessed using three standard measures of acoustic voice assessment: jitter, shimmer, and HNR.(21,37,39) Jitter is a measure of pitch instability (i.e., the sung note wavers in tone). A dysphonic singer will usually have more jitter than a healthy singer unless the healthy singer is intentionally wavering their tone for style (i.e., vibrato). Jitter has a typical value of variation 0.5–1% for sustained phonation in young adults.(47) Shimmer also measures instability but refers to wavering loudness. More shimmer is expected in a dysphonic voice than in a non-dysphonic voice. Shimmer values < 3% are considered normal for adults.(47) HNR, measured in decibels, is a measure of periodic signal in the voice (i.e., pure tone) compared to aperiodic noise (e.g., hissing). Some degree of friction or tension in the vocal tract, as seen in dysphonia, should generate lower HNR.(30) An HNR value < 7 dB is considered abnormal.(47) For this measure, the client sustained the vowel /a/ (i.e., rhymes with Ma) “at a comfortable pitch and loudness” for at least 4 s.
Loudness: Loudness was selected as an outcome measure associated with breath support and connected to glottal efficiency. The subject was instructed to “take a full breath and produce the vowel /a/ as loud as he can for at least 5 s.” Three opportunities, with 1-min breaks for recovery, were averaged to create a single loudness value for each assessment. Loudness data, measured in dB, were collected using a self-calibrating Sper 840029 Type 2 digital sound level meter (Sper Scientific Ltd., Scottsdale, AZ, USA).
Vocal range: Vocal range refers to the range of pitches the voice can accurately produce and is correlated with vocal efficiency and respiratory function.(48) Starting with middle C on the piano (i.e., C4), the subject was asked to sing a simple scale of five notes (e.g., do-re-mi-fa-so) using the vowel /a/. First, moving up the keyboard until he reached the upper limit of his range (i.e., his voice demonstrated break/fry) and then down the keyboard from C4 until he reached his lower limit.
Aerodynamic outcome measures
Maximum phonation time (MPT): MPT assesses the ability to continuously sustain vibration of the vocal folds (i.e., phonate) in a single breath (e.g., as when holding a note while singing). MPT was chosen because it provides a simple indicator of respiratory endurance and coordination with glottal efficiency while singing, both of which may be affected in a singer experiencing behavioral dysphonia. The client was instructed to “take a breath and sustain the vowel /a/ at a comfortable loudness and pitch, for at least 4 seconds.” Three opportunities, with 1-min breaks for recovery, were measured with a stopwatch and averaged to create a single MPT value for each assessment.
Peak expiratory flow (PEF): PEF, measured in liters per minute (L/min), is the maximum speed one can exhale air from the lungs following a full breath and has been found to be higher in experienced singers.(36) PEF was measured using a SpiroLink Model B1 handheld spirometer (CMI Health Inc., Alpharetta, GA, USA). The client was instructed to “take a breath and exhale as fast as possible until he had no air left to give.” A 1-min rest period was given between each trial. Data were manually recorded from the light emitting diode (LED) screen of the SpiroLink following each trial. The three trials were then averaged.
Subjective outcome measure
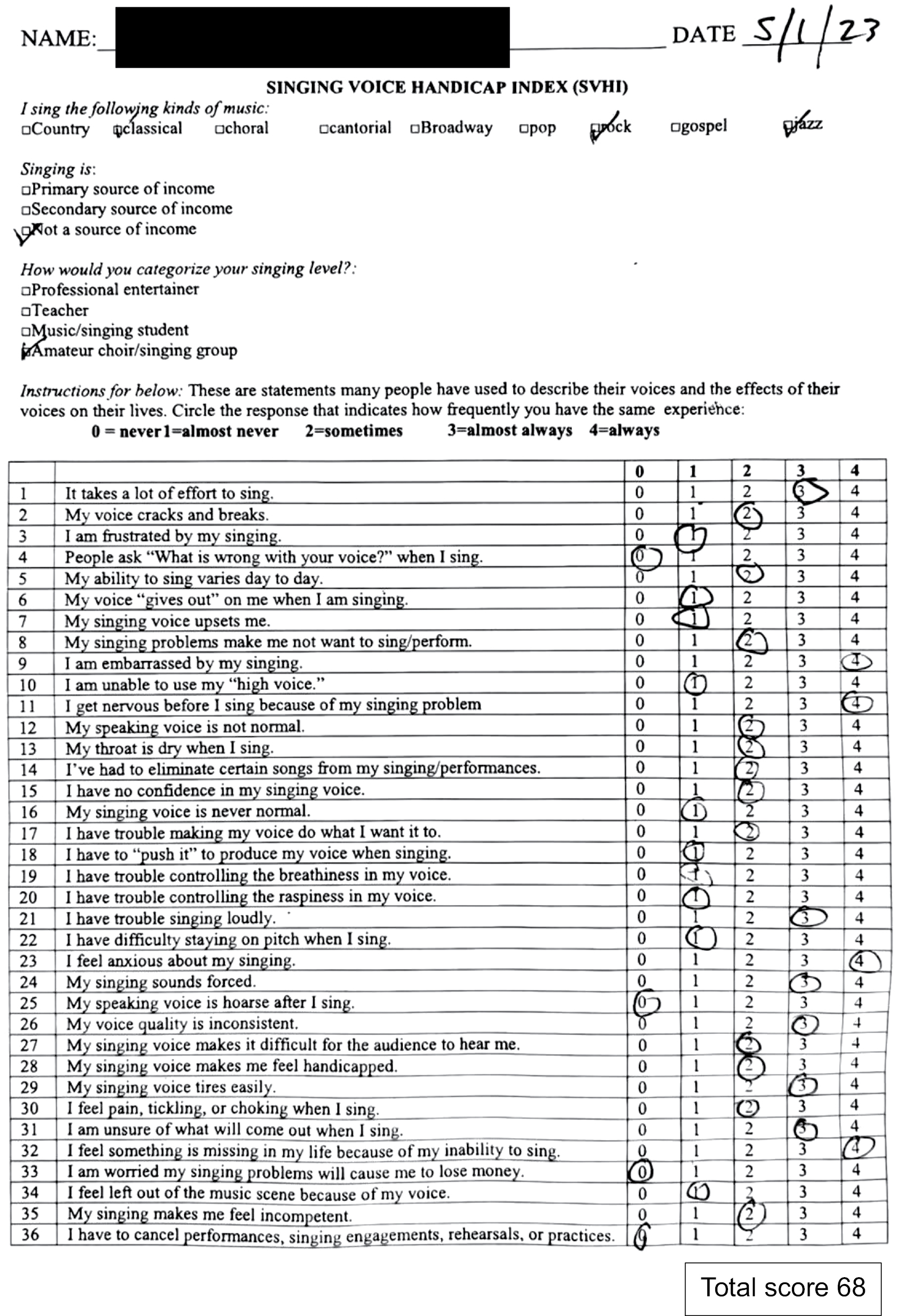
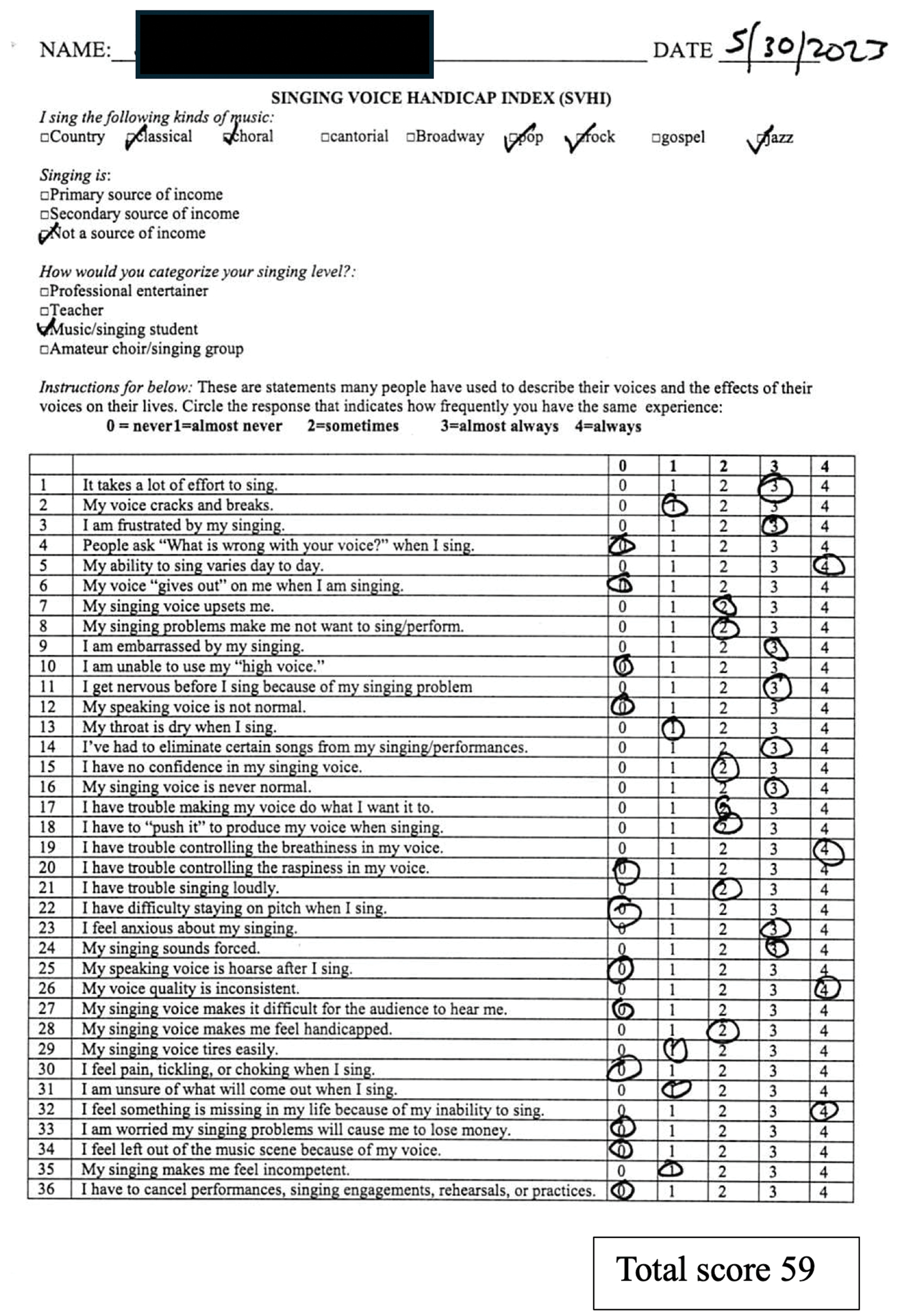
Singing Voice Handicap Index (S-VHI): Immediately following instrumental analysis of voice, the client completed the S-VHI, a validated self-assessment questionnaire. The S-VHI measures the perceived functional, physical, and emotional impact a voice condition has on a singer’s performance and quality of life.(35) Thirty-six statements are rated on a 0–4 scale (i.e., 0—never; 1—almost never; 2—sometimes; 3—almost always; and 4—always) to generate a total S-VHI score. A higher score indicates a greater perceived handicap (see Appendix A and B). The mean normative value of the S-VHI is 20.35.(49)
Functional singing assessment
To assess the effect of treatment in a functional context, the client sang a 2-min 45-s song of his choice to a karaoke track played through headphones. The song was performed in the key of D major and had a pitch range from C#3 to D5. Functional vocal range, HNR, and breath fluency were assessed. The procedures and equipment for acoustic data collection were the same as previously described. Data were recorded at baseline before any treatment had begun and on the final day following the final massage session.
Functional vocal range: Functional vocal range refers to the client’s vocal range while performing a song.
Functional HNR: Functional HNR refers to the average HNR across a song. Data were collected in increments of 10 s or less and averaged across each recording.
Breath fluency: Breath fluency, a measure developed for this study, is defined here as breaths taken during singing without unnecessary interruptions, gasping inhales (i.e., a sudden sharp gasp despite adequate time for fluent inspiration between phrases), vocal artifacts (i.e., throat clearing or abandoned phrases), or quick rapid gasps (e.g., as if panting).
Client journal
To provide a client perspective and insight into treatment effects, and aid interpretation of results for discussion, the client was instructed to keep a journal reflecting on his therapy experience and his perception of any change. No schedule or specific format was implemented.
The massage therapist who conducted the study was also a licensed speech–language pathologist with advanced training in vocal habilitation and was professionally experienced with vocal assessment and treatment. At the time of the report, he was completing his final weeks of massage study at HACC.
Informed consent
Following an educational overview and open discussion, the client provided informed consent to participate in this case study, including the use of anonymized data and images in publication. The consent process adhered to ethical guidelines and included a detailed discussion of treatment approaches, goals, and the client’s right to withdraw at any time.
Procedure
A total of six 90-min massage therapy sessions were performed across 4 weeks (i.e., Mondays and Wednesdays) with a 1-week break on the second week when the client was not available. The 90-min session duration allowed sufficient time to address all targets of the treatment protocol. A treatment frequency of two sessions per week was chosen as a manageable balance between client availability, treatment frequency, and ongoing assessment of both immediate and cumulative treatment effects.
To assess immediate treatment effects, all outcome measures were assessed before and after each session, except vocal range, visual breath/posture, and functional singing. The latter were assessed only at baseline and after the final session, as these were anticipated to change more gradually and reflect cumulative rather than immediate progress.
The treatment plan was designed following a thorough review of the body and voice literature. Each component of the vocal system was mapped and targeted per the manually accessible anatomy of its subsystems (i.e., respiration, phonation, resonance, articulation) as well as that of posture.(2,4,9–11,13,15,25,34,43,44,50–52) Direct laryngeal manipulation was excluded to highlight the integrative nature of the vocal system outside the larynx. For details of the treatment plan and procedure, see supine position (Table 2), followed by prone position (Table 3). During treatment, areas of hypertonicity possibly contributing to restriction of the vocal system were identified with thoughtful palpation,(33) then addressed until palpable release with fascial work and professional massage techniques performed with moderate to deep pressure.(33) Before the therapist left the massage room following each session, he encouraged the client to vocalize privately however he desired. This never lasted more than 2 min, including the time for the client to dress.
Table 2. Treatment Plan—Supine Position
| Position | Modality | Anatomy | Technique |
|---|---|---|---|
| Supine | Connective tissue | Area of C7 to occiput, upper trapezius followed to acromion, medial chest to shoulder along clavicular border, xiphoid process to clavicle | Sink into tissue with flat hands. Gentle stretch into tissue resistance until release. |
| Connective tissue | Infrahyoid space (manubrium to hyoid) and suprahyoid space (hyoid to anterior aspect of mandible) | Open, flat-fingered grip molded to space. Gentle stretch into resistance of tissue until release. | |
| Connective tissue | Tongue | Fold gauze over protruded tongue. Gently stretch surface tissue anteriorly with thumbs until gradual release. | |
| Stretch | Sternocleidomastoid (SCM), scalenes, levator scapulae, longus colli, splenius capitis, splenius cervicis | Lateral head tilt. Stretch to opposite shoulder. | |
| Swedish | SCM | Stripping with extended thumb and fist using controlled head rocking. | |
| Masseter | Raking origin to insertion, then static fingertip hold with instruction to open mouth into /ah/ position. Hold 3 s (performed proximal, intermediate, and distal to origin). | ||
| Genioglossus | Raking insertion to origin. | ||
| Scalenes | Intentional touch following direction of origin to insertion. | ||
| Upper trapezius | Soft fist stroking. | ||
| Pectoralis major and minor, subclavius | Stripping, raking, and pin and stretch facilitated with arm movement. | ||
| External intercostals | Lateral to medial tracing/raking with fingertips. | ||
| Transverse abdominus and obliques | Lateral to medial raking. | ||
| Diaphragm | Sink into anterior costal origins with flat fingertips. Depth gained following motion of deep breath (instructed). |
Table 3. Treatment Plan—Prone Position
| Position | Modality | Anatomy | Technique |
|---|---|---|---|
| Prone | Swedish | Abdominals | Raking from lateral to medial. |
| Lower erectors | Cross-fiber stroking with flat surface of bladed fingertips. | ||
| Quadratus lumborum | Bladed hands, index fingers together in diving position using thumbs leveraged together to locate and stroke muscle belly. | ||
| Latissimus dorsi | Flat hand wringing from sacral origin toward insertion with fist kneading toward insertion using arm movement for access. | ||
| Upper trapezius | Raking and stroking compression in hands. | ||
| Levator scapulae | Soft fist stroking from origin toward insertion. | ||
| Supraspinatus | Raking with fingertips medial to lateral. | ||
| Serratus posterior superior, splenius capitis, erector group | Soft fist kneading. | ||
| Scalenes | Gentle raking with fingertips. | ||
| Suboccipitals | Raking and circular stroking. |
Visual posture/breath assessment
Posture: As shown in Figure 1 and Table 4, forward head posture, cervical hyperlordosis, and thoracic hyperkyphosis decreased overall. The client’s shoulders relaxed inferiorly from their elevated position above the clavicle before treatment. Also note that post-treatment image shows apparent infrahyoid release with larynx relaxed from an inferior posture and a more neutral position of laryngeal prominence and cricoid cartilage.
Figure 1. Posture pre–post treatment (face blurred for privacy).
Table 4. Results of Postural Assessment
| Pre-Massage Therapy | Post-Massage Therapy |
|---|---|
| Cervical hyperlordosis and thoracic hyperkyphosis present. | Hyperkyphosis and hyperlordosis slightly normalized. |
| Elevated shoulders. R higher than lower. | Shoulders relaxed inferiorly. L still higher. |
| Prominent thyroid cartilage/laryngeal position. | Larynx relaxed in position. |
Breath: At baseline during a “comfortable deep breath,” the client demonstrated thoracic engagement including some extension of head and neck and elevation of shoulders. After the final treatment, the client allowed anterior abdominal wall to expand without observed compensatory thoracic/head/neck or shoulder engagement (Table 5).
Table 5. Results of Visual Breath Assessment
| Pre Massage Therapy | Post Massage Therapy |
|---|---|
| Slightly effortful extension of neck and elevation of head during inspiration. | No head/neck movement observed. |
| Slight elevation of the head and shoulders during inspiration. | No head/shoulder movement observed. |
| Slightly effortful thoracic engagement during inspiration. | No thoracic movement. Allowed anterior abdominal wall to relax and expand to promote diaphragmatic depression. |
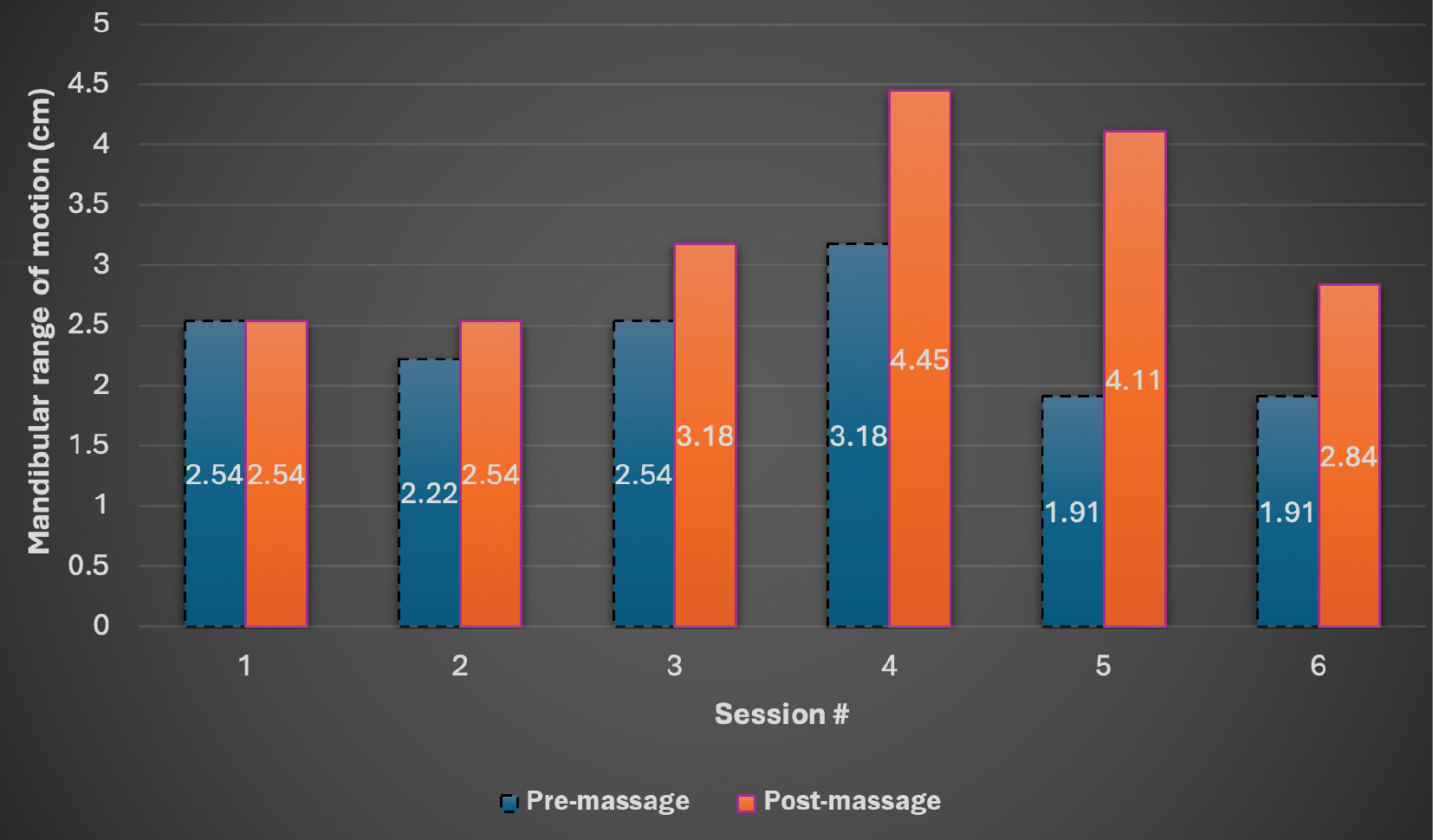
Mandibular ROM: Jaw opening increased following every session, except session 1, where it remained the same. By the following session, however (except session four), jaw opening had returned to near or below baseline of 2.54 cm. Note maximum increase from 1.91 cm to 4.11 cm (2.2 cm total) pre–post treatment session 5 (see progress in Figure 2).
Figure 2. Mandibular range of motion.
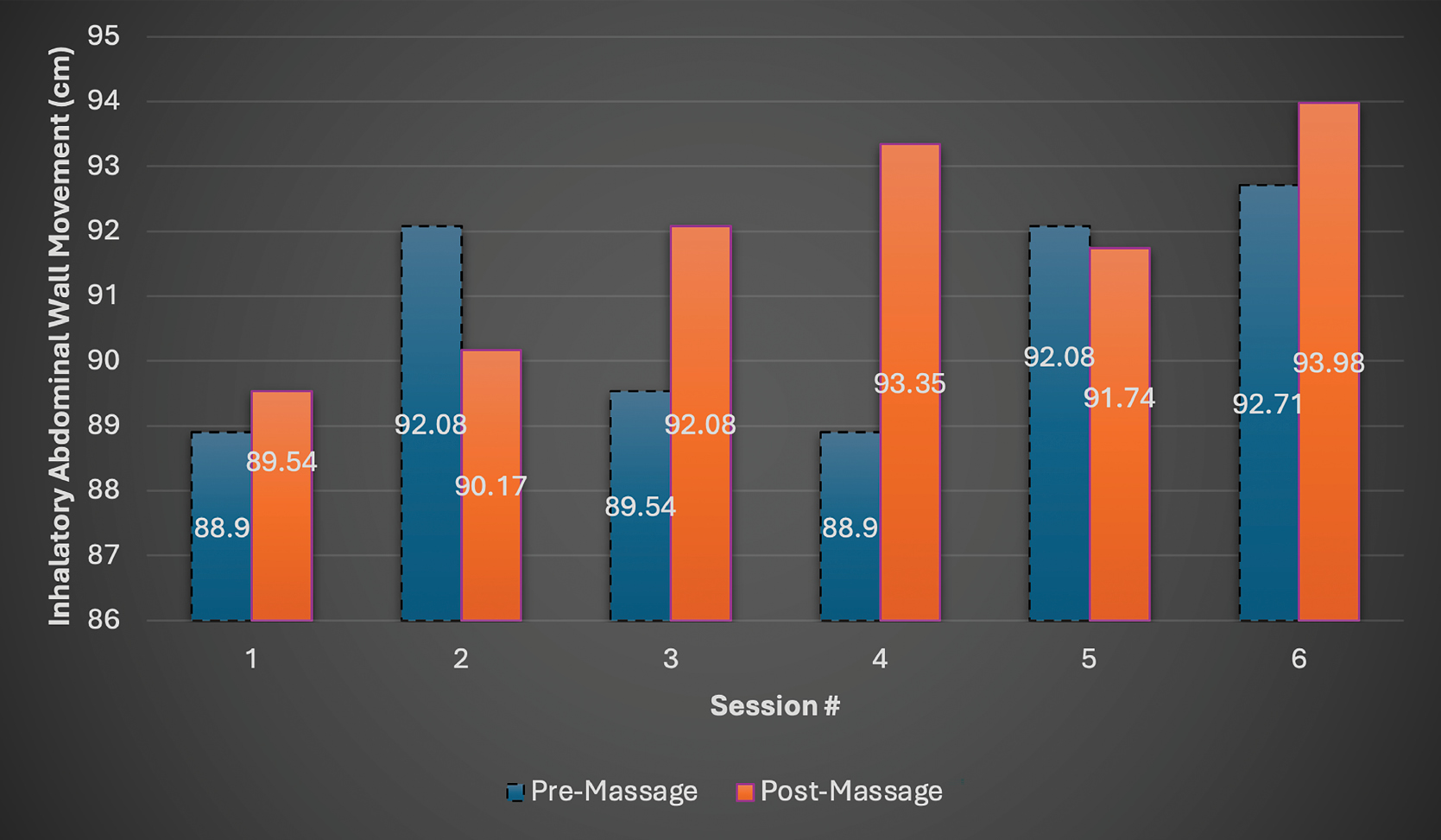
Inspiratory abdominal wall movement: Inspiratory abdominal wall movement increased from a baseline of 88.9 cm to a measurement of 92.71 cm before and 93.98 cm after the final session. Pre–post session outcomes were inconsistent as seen in Figure 3.
Figure 3. Inhalatory abdominal wall movement.
Acoustic outcome measures
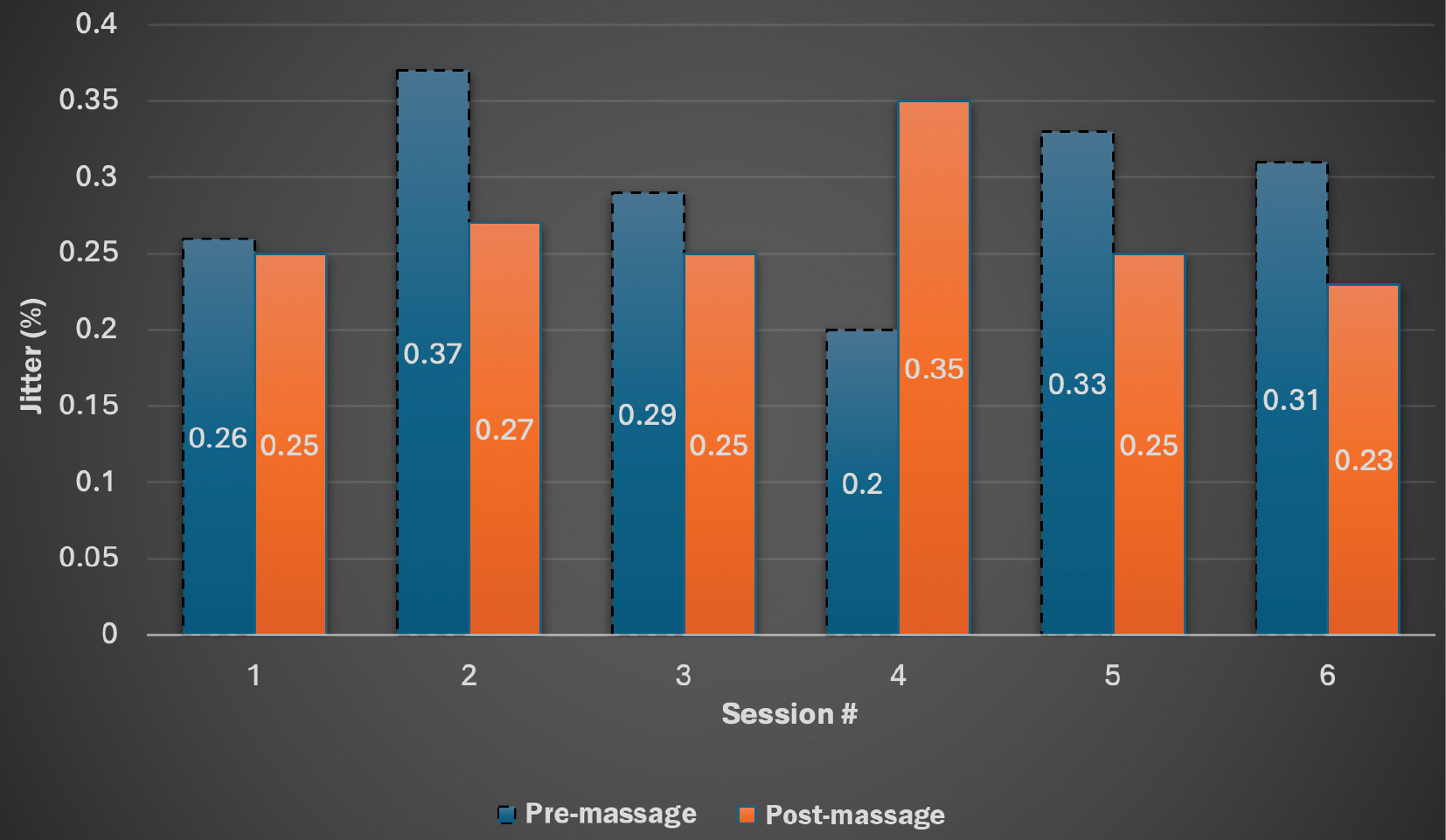
Jitter: While values remained within functional limits (<0.5%), in response to treatment, jitter consistently decreased following all sessions except session 4 but did not maintain a consistent pre-treatment measure below baseline (see progress in Figure 4).
Figure 4. Jitter.
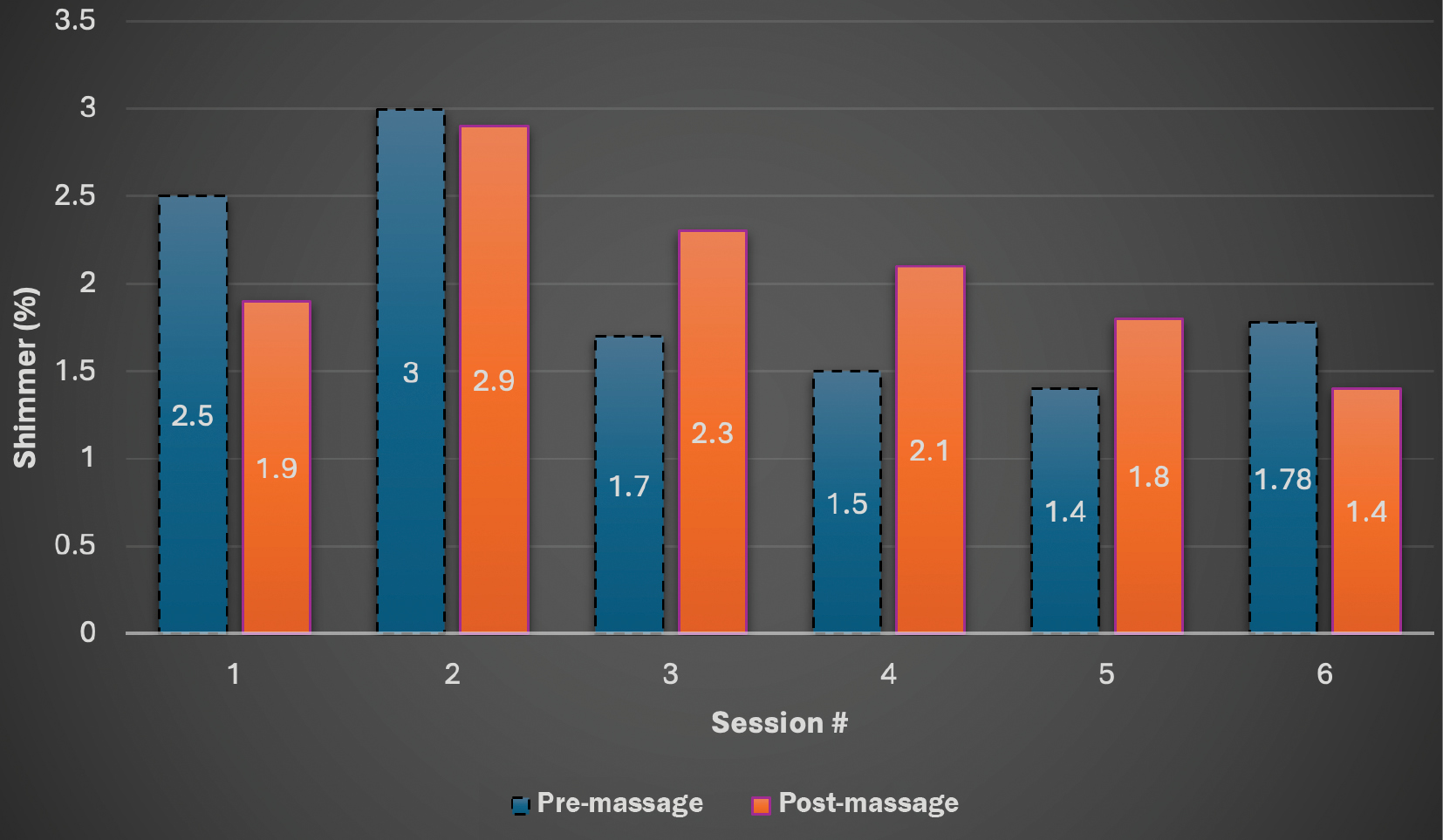
Shimmer: Shimmer was consistently within functional limits (<3%). In response to treatment, values decreased from 2.5% at baseline to 1.78% before and 1.4% after final session. Pre–post session outcomes were not consistent as demonstrated in Figure 5.
Figure 5. Shimmer.
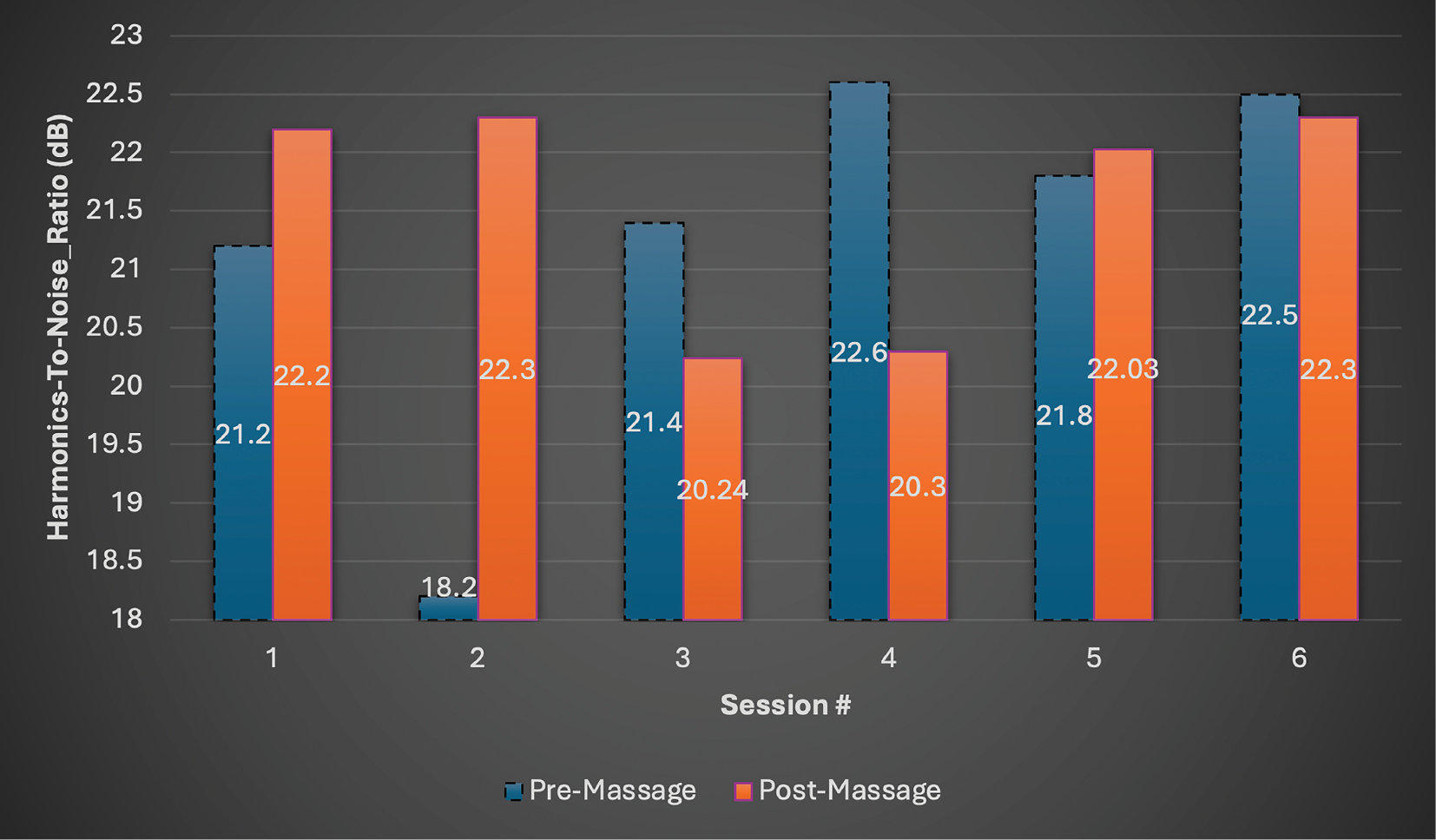
HNR: HNR remained in a healthy range well above 7 dB. Following the final session, HNR increased from 21.2 dB at baseline to 22.5 dB pre-treatment and 23.3 dB post-treatment final session. Inconsistent pre–post session outcomes are illustrated in Figure 6.
Figure 6. Harmonics-to-noise ratio (HNR).
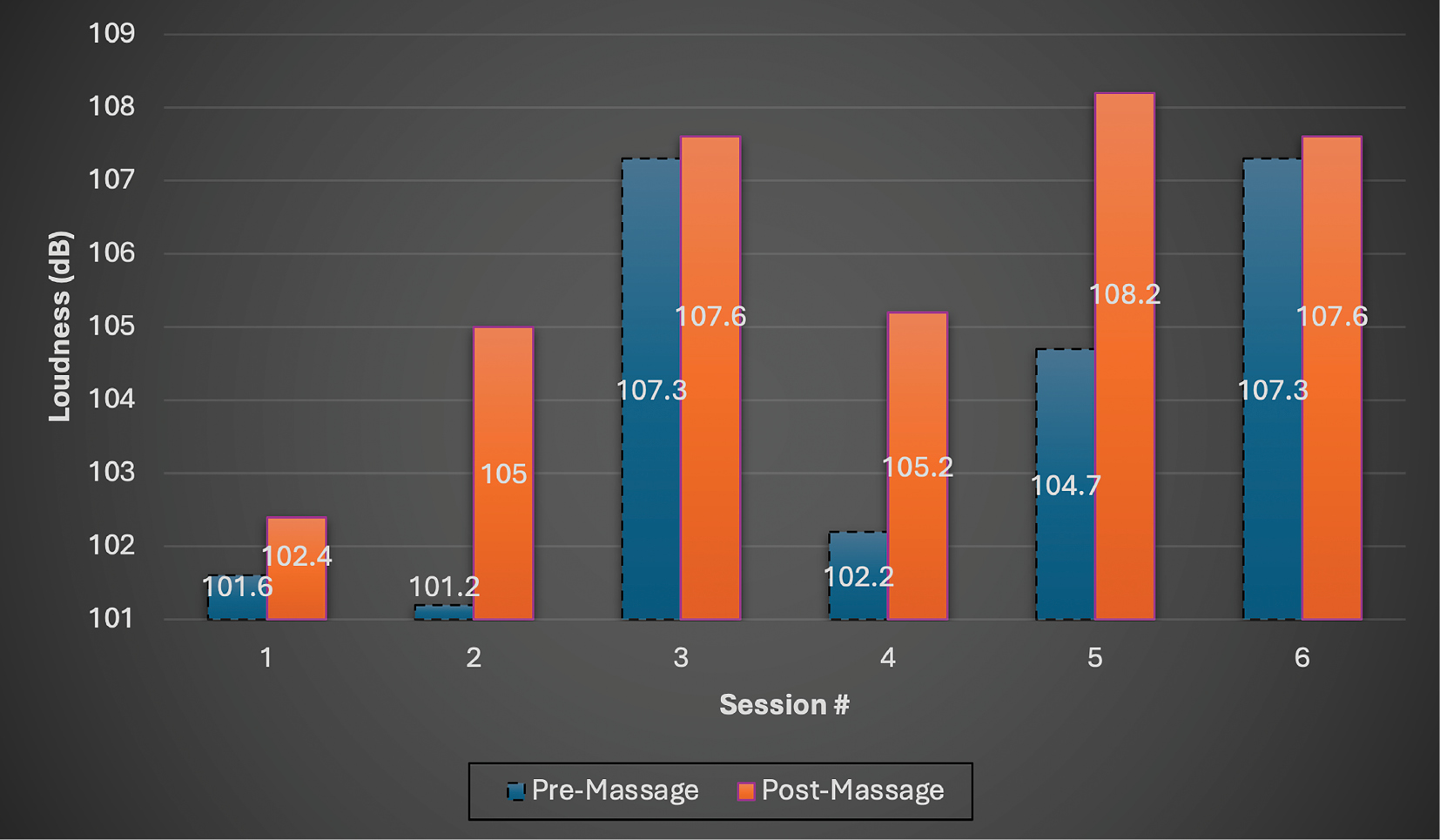
Loudness: Loudness increased by 6 dB from 101.6 dB at baseline to 107.3 dB pre and 107.6 dB post final session. A consistent pre–post session increase was also demonstrated (see progress in Figure 7).
Figure 7. Loudness.
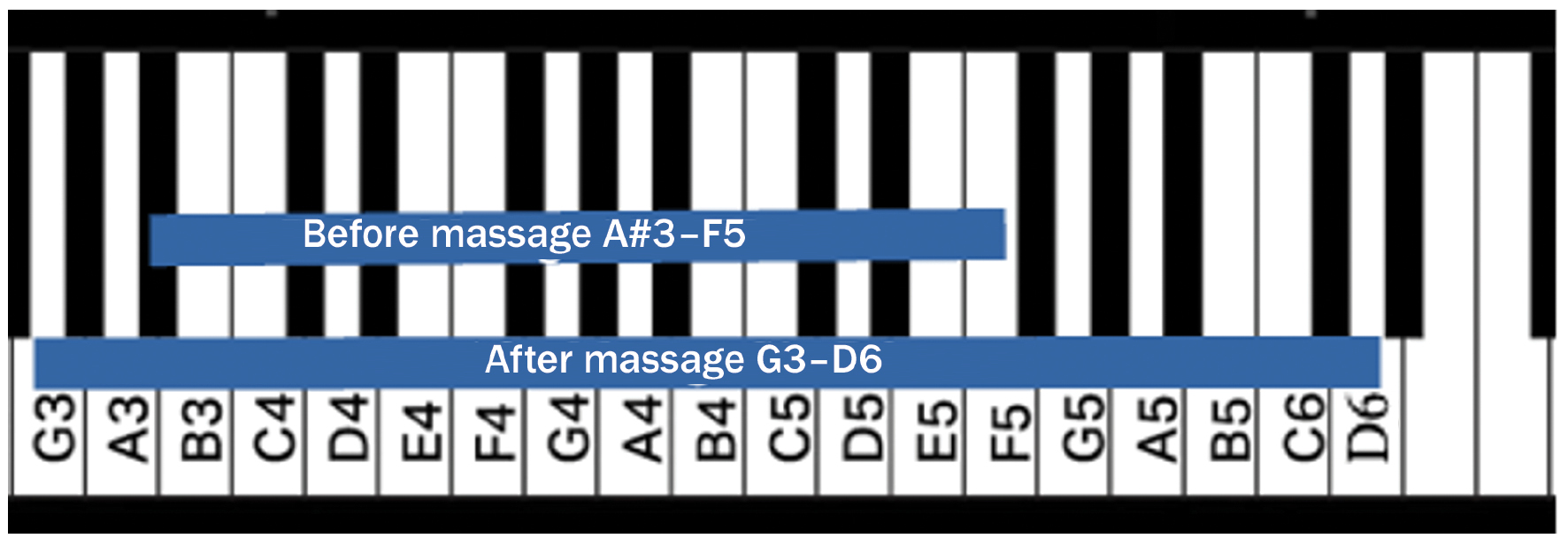
Vocal range: Vocal range increased by six whole tones (i.e., three semitones in the lower range (A#3–G3) and nine semitones in the upper range (F5–D6)) (see Figure 8).
Figure 8. Vocal range pre–post treatment.
Aerodynamic outcome measures
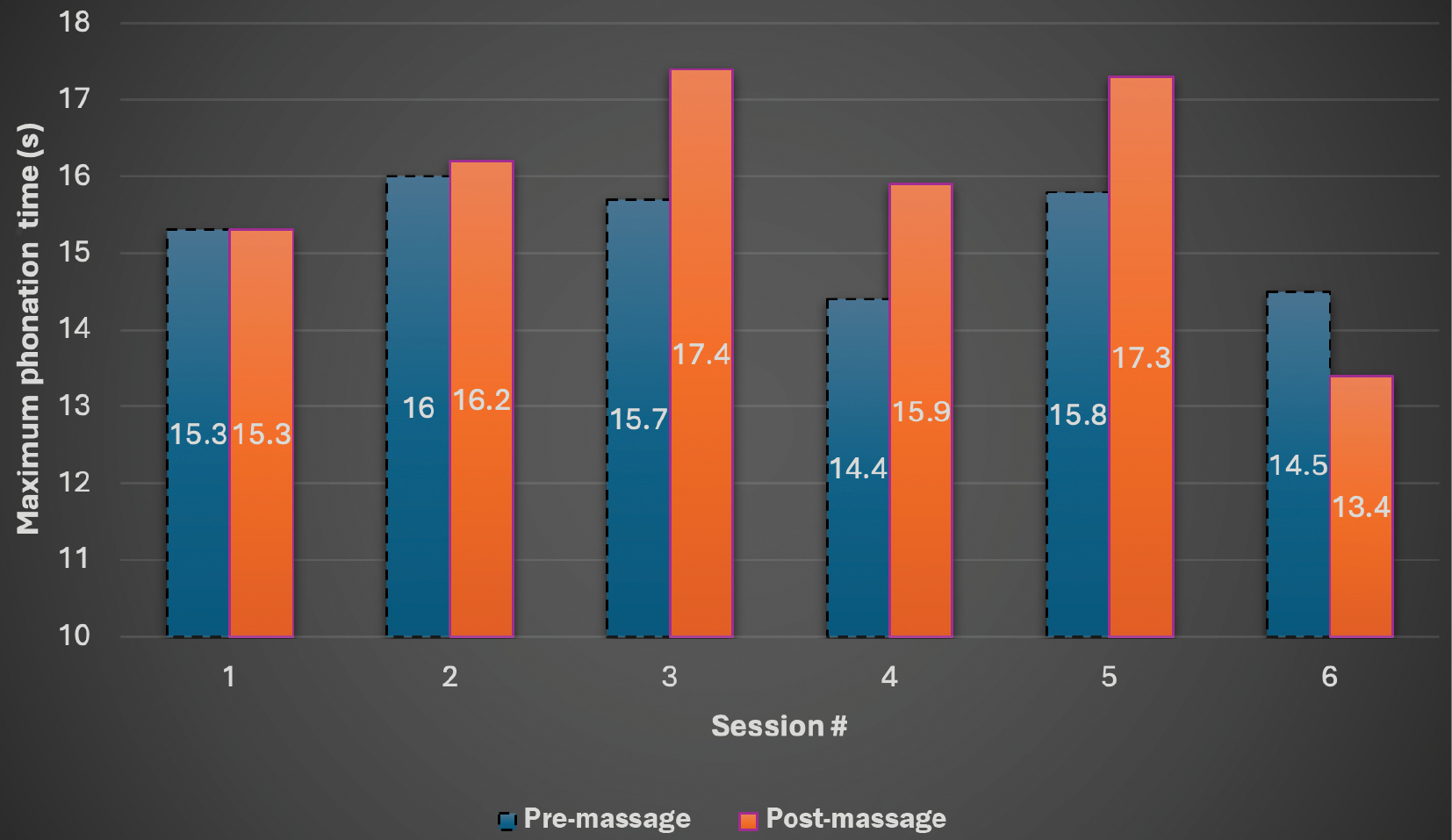
Maximum phonation time: Despite a post-session increase across the treatment course, following the final session the client’s ability to sustain phonation (i.e., MPT) was below both baseline and pre-session measures (see progress in Figure 9).
Figure 9. Maximum phonation time (MPT).
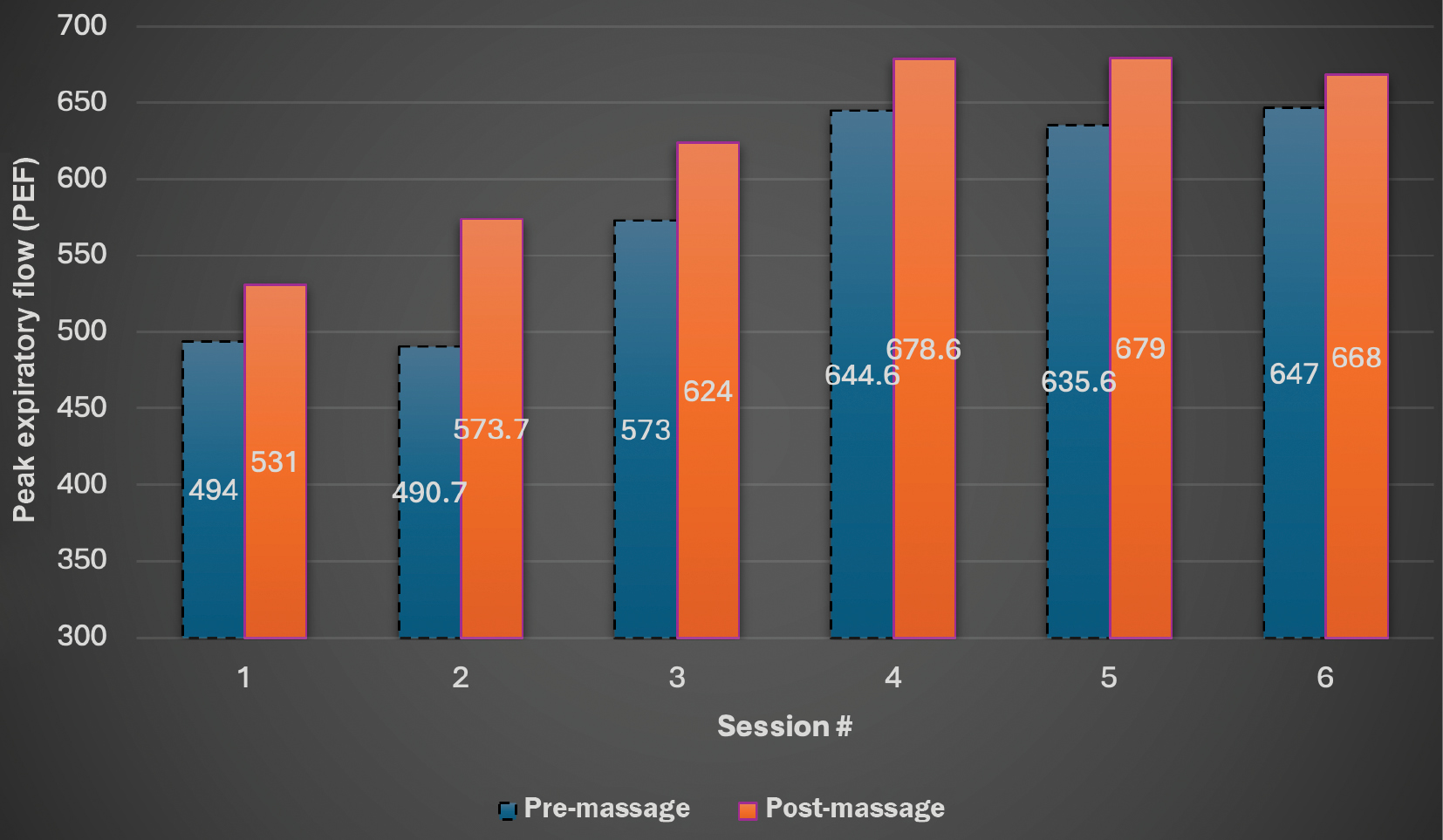
Peak expiratory flow: PEF increased from 494 L/min at baseline to 647 L/min pre and 668 L/min post final session. A consistent increase was also observed pre–post individual session (see progress in Figure 10).
Figure 10. Peak expiratory flow (PEF).
Subjective outcome measures
Singing Voice Handicap Index: The normative value for the Singing Voice Handicap Index is 20.35. The client scored 68 during the initial evaluation and 59 following the final session (see Appendix A and B). This 9-point decrease remains 38–39 points higher than the normative range, indicating that the client continues to perceive a voice handicap.
Functional singing assessment
Functional vocal range: Functional vocal range increased by one octave to D5 sung in falsetto. Before treatment, the client sang this note an octave lower in chest voice.
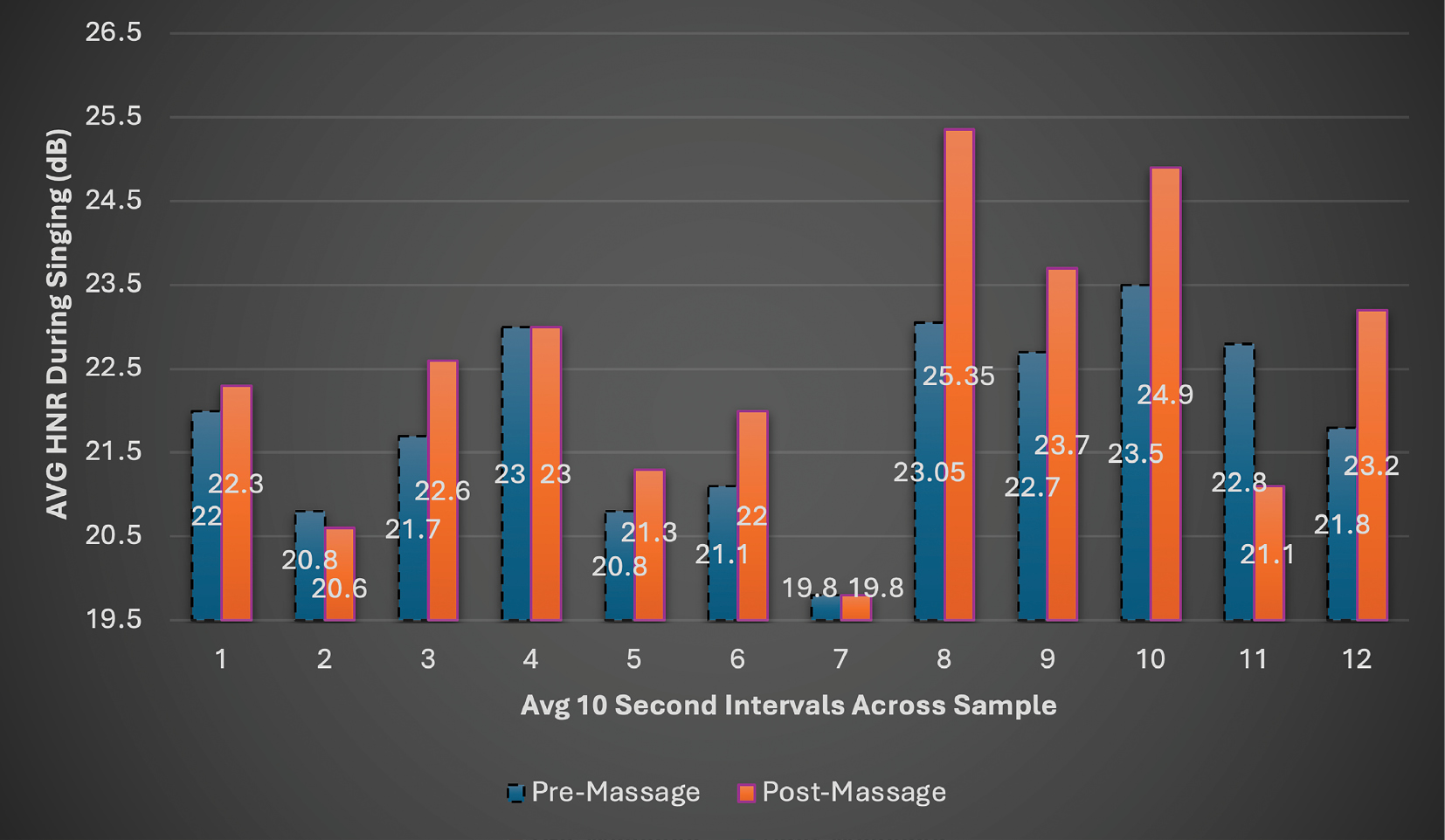
Functional HNR: Average HNR during the singing sample increased by 0.68 dB from 21.8 dB pre to 22.48 dB post treatment (see Figure 11 to compare data across the whole song).
Figure 11. AVG HNR during singing.
Breath fluency: Before treatment, the client demonstrated 25 balanced breaths, 6 gasping breaths, 2 quick double breaths (i.e., panting), 2 throat clears, and 1 abandoned phrase before a double breath. Following the final treatment session, the client demonstrated 30 balanced breaths with only 3 gasping breaths and 0 artifacts (i.e., throat clears, abandoned phrases).
This case report explored the effects of a massage protocol targeting hypertonicity in the vocal system, without direct laryngeal manipulation, exercises, or training, on a singer with symptoms of behavioral dysphonia. Due to the integrative nature of voice production as a whole-body phenomenon, it was hypothesized that vocal symptoms would improve, despite the larynx itself receiving only incidental contact.
Informed by research identifying the role of posture on the vocal system,(10,12,14) postural anatomy was addressed. Though laryngeal contact was indirect, the client’s laryngeal position appeared to neutralize from an inferiorly pulled posture. Shoulder elevation decreased and thoracic hyperkyphosis and cervical hyperlordosis were reduced. The client noted in his treatment journal: “…(massage) led to sitting and standing up straight more comfortably, and my family has even noticed this and commented on it.” Informed by the science of respiratory function in singing,(9,44,48,51) the accessible primary and secondary muscles of respiration were addressed. By the final session, PEF, a recognized outcome for singers,(36) increased from baseline by 174 L/min post treatment and abdominal ROM increased by 5 cm. Following the final session, the client journaled: “I was connected with the deep breaths in my diaphragm, and the breath being unobstructed traveling throughout my body. It felt like a constant stream that I could control with a valve.” An entry after session 3 included: “When holding a note it was just one continuous stream of air with no effort really.” Because restricted articulation is associated with dysphonia,(15) the treatment plan addressed the masseter muscles. Though ROM consistently improved pre–post session, it was 0.63 cm below baseline pre treatment on the final day. Led by the concept of “muscle interaction,”(33) where tension in one structure can cause compensatory tension patterns in adjacent muscles, muscles of the head and neck were addressed to affect the vocal and pharyngeal anatomy. Less compensatory thoracic/head/neck movement when singing followed. Vocal range increased by six whole tones, and functional vocal range during singing improved to a D5 sung in falsetto (originally sung an octave lower in chest voice). Loudness increased by 6 dB, and MPT increased following every session, except the final session. Though acoustic measures (i.e., jitter, shimmer, and HNR) were always within normal limits and varied from session to session, jitter improved post treatment in most sessions and shimmer and HNR showed some improvement from baseline by the final session. Functional HNR and breath fluency both improved during the singing task.
The client’s S-VHI score, though improved by 9 points, remained above normative values indicating a continued perception of voice handicap (see Appendix A and B). In his final journal entry, the client reported, “I have ranked some questions on the Singing Voice Handicap Index more negatively, but I believe that is due to becoming more aware of my abilities and what I need to improve upon.” This aligns with the specifics of his responses. Some scores reflecting awareness of ability increased (e.g., “my singing voice is never normal,” “I have trouble…,” “… quality is inconsistent”). Meanwhile, perception of many physical symptoms likely addressed by massage (e.g., fatigue, pain, dry throat, choking, “voice giving out”) decreased to zero or near zero.
As visualized in Figures 2–8, aside from PEF, which demonstrated a smooth and gradual trend of progress post session (see Figure 10), some outcomes reflected inconsistent progress between and within sessions. There are notable patterns within this variability. By the final session, five out of eight outcomes (i.e., abdominal wall movement, shimmer, HNR, loudness, and PEF) improved from baseline on all but one session, typically session 2. The client noted: “I noticed on days that I was stressed or nervous due to outside circumstances, I had more trouble singing and producing quality sound. After seeing the results, I felt like you could see the days I was more stressed.” This does not explain all of the variability but illuminates the holistic nature of voice as a function of the whole person, including emotion, stress, personality, and body.(19–21) Despite variability, all outcomes, except HNR and shimmer, demonstrated mostly consistent pre–post session improvement.
As a single-subject case report without a control group, these findings are not conclusive. There was also a potential for bias as the clinician was the sole evaluator and the client’s perceived expectations of benefit could have influenced his performance (i.e., subject bias).
This case demonstrated that following a therapeutic massage protocol targeting hypertonicity in the vocal system without direct laryngeal manipulation, or vocal exercises/training, vocal function improved for a client with symptoms of behavioral dysphonia. Despite variability, immediately following most sessions, jaw movement, phonation time, breath flow, loudness, and jitter improved. By the final session, loudness increased by 6 dB and vocal range increased by six whole tones. During functional singing, breath fluency, HNR, and vocal range had all improved following the treatment course.
This report adds to the limited number of studies merging the practices of professional massage therapy and clinical voice care. Although the human voice is a whole-body phenomenon, future controlled research should identify specific mechanisms, targets, and methods for optimal release of vocal restriction while taking the whole body into account. It is hoped that such investigations continue to inspire interdisciplinary collaboration, harmonizing the clinical knowledge and expertise of voice care professionals with the therapeutic insight and skilled touch of licensed massage therapists. As the evidence base in this area of research continues to grow, the clinical value that licensed massage therapists offer to the voice care team may be increasingly recognized in professional practice. In such a paradigm, specially trained massage therapists can assess the whole body and release physical restriction affecting the vocal system at baseline, helping voice pathologists and their patients proceed to voice therapy with less physical obstacles in their way.
I want to thank my mentor Nina Kottcamp, LMT, for her kind support, thoughtful guidance, and selfless encouragement. I am thankful to Chris Purcell for connecting me with a person in need. I want to thank Barb Stockland, for her valuable research support. And to my Lord and Savior Jesus Christ, who set me on this path to help and guide others to heal.
The author declares there are no conflicts of interest.
No sources of funding were used in this study.
1. Ribeiro VV, Pedrosa V, Silverio KCA, Behlau M. Laryngeal manual therapies for behavioral dysphonia: a systematic review and meta-analysis. J Voice. 2018;32(5):553–563. [CrossRef] [PubMed]
2. Ribeiro VV, de Oliveira AG, da Silva Vitor J, Siqueira LTD, Moreira PAM, Brasolotto AG, et al. The effect of a voice therapy program based on the taxonomy of vocal therapy in women with behavioral dysphonia. J Voice. 2019;33(2):256.e1–256.e16. [CrossRef] [PubMed]
3. Aronson AE. Clinical Voice Disorders: An Interdisciplinary Approach. 3rd ed. Thieme; 1990.
4. Desjardins M, Apfelbach C, Rubino M, Verdolini Abbott K. Integrative review and framework of suggested mechanisms in primary muscle tension dysphonia. J Speech Lang Hear Res. 2022;65(5):1867–1893. [CrossRef] [PubMed]
5. Roy N, Ford CN, Bless DM. Muscle tension dysphonia and spasmodic dysphonia: the role of manual laryngeal tension reduction in diagnosis and management. Ann Otol Rhinol Laryngol. 1996;105(11):851–856. [CrossRef] [PubMed]
6. Roy N. Assessment and treatment of musculoskeletal tension in hyperfunctional voice disorders. Int J Speech Lang Pathol. 2008;10(4):195–209. [CrossRef] [PubMed]
7. Dehqan A, Scherer RC. Positive effects of manual circumlaryngeal therapy in the treatment of muscle tension dysphonia (MTD): long term treatment outcomes. J Voice. 2019;33(6):866–871. [CrossRef] [PubMed]
8. Ahmadi N, Abbott KV, Rajati F, Khoddami SM, Torabinezhad F, Ebrahimi Takamjani I, et al. Effects of laryngeal manual therapy on primary muscle tension dysphonia (MTD-1): implications for MTD-1 type. J Voice. 2024;38(6):1377–1385. [CrossRef] [PubMed]
9. Rubin JS, Macdonald I, Blake E. The putative involvement of the transabdominal muscles in dysphonia: a preliminary study and thoughts. J Voice. 2011;25(2):218–222. [CrossRef] [PubMed]
10. Cielo CA, Christmann MK, Ribeiro VV, Hoffmann CF, Padilha JF, Steidl EMS, et al. Musculoskeletal stress syndrome, extrinsic laryngeal muscles and body posture: theoretical considerations. Síndrome de tensão musculoesquelética, musculatura laríngea extrínseca e postura corporal: considerações teóricas. Rev CEFAC. 2014;16(5):1639–1649. [CrossRef]
11. Gilman M, Johns MM. The effect of head position and/or stance on the self-perception of phonatory effort. J Voice. 2017;31(1):131.e1–131.e4. [CrossRef] [PubMed]
12. Cardoso R, Lumini-Oliveira J, Meneses RF. Associations between posture, voice, and dysphonia: a systematic review. J Voice. 2019;33(1):124.e1–124.e12. [CrossRef] [PubMed]
13. Gilman M. The influence of postural changes on extralaryngeal muscle tension and vocal production. Perspect ASHA Spec Interest Groups. 2018;3(3):82–87. [CrossRef]
14. Staes FF, Jansen L, Vilette A, Coveliers Y, Daniels K, Decoster W. Physical therapy as a means to optimize posture and voice parameters in student classical singers: a case report. J Voice. 2011;25(3):e91–e101. [CrossRef] [PubMed]
15. Roy N, Nissen SL, Dromey C, Sapir S. Articulatory changes in muscle tension dysphonia: evidence of vowel space expansion following manual circumlaryngeal therapy. J Commun Disord. 2009;42(2):124–135. [CrossRef] [PubMed]
16. Myers R. Dysphonia: a speech and language therapy perspective. J Bodw Mov Ther. 1999;3(3):126–133. [CrossRef]
17. Oliveira P, Cavalcante MEOB, Nascimento CA, Ribeiro VV. Factors predicting dysphonia in professional voice users. J Voice. 2025;39(1):178–184. [CrossRef] [PubMed]
18. Cardoso R, Lumini-Oliveira J, Meneses RF. Associations between autonomic nervous system function, voice, and dysphonia: a systematic review. J Voice. 2021;35(1):104–112. [CrossRef] [PubMed]
19. Faure MA, Perouse AR, Coulombeau B. Therapeutic choices for curing dysodia?…three clinical cases. Rev Laryngol Otol Rhinol (Bord). 2010;131(1):59–60. [PubMed]
20. Dahl KL, Stepp CE. Effects of cognitive stress on voice acoustics in individuals with hyperfunctional voice disorders. Am J Speech Lang Pathol. 2023;32(1):264–274. [CrossRef] [PubMed]
21. Erratum to “Effects of cognitive stress on voice acoustics in individuals with hyperfunctional voice disorders.” Am J Speech Lang Pathol. 2023;32(2):813. [CrossRef] [PubMed]
22. da Cunha Pereira G, de Oliveira Lemos I, Dalbosco Gadenz C, Cassol M. Effects of voice therapy on muscle tension dysphonia: a systematic literature review. J Voice. 2018;32(5):546–552. [CrossRef] [PubMed]
23. Goffi-Fynn JC, Carroll LM. Collaboration and conquest: MTD as viewed by voice teacher (singing voice specialist) and speech-language pathologist. J Voice. 2013;27(3):391.e9–391.e14. [CrossRef] [PubMed]
24. Flock L, King SR. A manual therapy in need of a manual: conceptualizing and comparing existing vocal massage protocols and their use in the treatment of voice problems. Voice Speech Rev. 2023;18(3):348–361. [CrossRef]
25. Mathieson L, Hirani SP, Epstein R, Baken RJ, Wood G, Rubin JS. Laryngeal manual therapy: a preliminary study to examine its treatment effects in the management of muscle tension dysphonia. J Voice. 2009;23(3):345–353. [CrossRef] [PubMed]
26. Salehi A, Barkmeier-Kraemer J. Laryngeal manual therapy as a treatment for impaired production of Tahrir vibrato in traditional Iranian singers. Folia Phoniatr Logop. 2014;66(6):265–272. [CrossRef] [PubMed]
27. Ahmadi N, Abbott KV, Rajati F, Moein N, Khoddami SM, Torabinezhad F, et al. Effectiveness of edge therapy: a randomized clinical trial for muscle tension dysphonia. J Voice. 2025. In press. [CrossRef] [PubMed]
28. Boominathan P, Mahalingam S, Arunachalam R, Venkatesh L. An eclectic voice therapy program for the treatment of hyperfunctional voice disorders (HFVD). J Voice. 2023;37(6):969.e1–e21. [CrossRef] [PubMed]
29. Hockey K, Kennedy E. The role and impact of voice physiotherapy: a qualitative study of service user perspectives. Physiother Theory Pract. 2025;41(4):783–791. [CrossRef] [PubMed]
30. Laukkanen AM, Leppänen K, Tyrmi J, Vilkman E. Immediate effects of ‘voice massage’ treatment on the speaking voice of healthy subjects. Folia Phoniatr Logop. 2005;57(3):163–172. [CrossRef] [PubMed]
31. Leppänen K, Laukkanen AM, Ilomäki I, Vilkman E. A comparison of the effects of voice massage and voice hygiene lecture on self-reported vocal well-being and acoustic and perceptual speech parameters in female teachers. Folia Phoniatr Logop. 2009;61(4):227–238. [CrossRef] [PubMed]
32. Ternström S, Andersson M, Bergman U. An effect of body massage on voice loudness and phonation frequency in reading. Logop Phoniatr Vocol. 2000;25(4):146–150. [CrossRef] [PubMed]
33. Beck MF. Theory & Practice of Therapeutic Massage. 4th ed. Clifton Park, NY: Thomson Delmar Learning; 2006.
34. Gilman M. Body and Voice: Somatic Re-Education. Plural Publishing, Inc.; 2014.
35. Cohen SM, Jacobson BH, Garrett CG, Noordzij JP, Stewart MG, Attia A, et al. Creation and validation of the Singing Voice Handicap Index. Ann Otol Rhinol Laryngol. 2007;116(6):402–406. [CrossRef] [PubMed]
36. Shirke DRS, Killedar DR. Peak expiratory flow rate in Indian female classical singers. Int J Recent Adv Multidiscip Res. 2019;6(3):4772–4774.
37. Lundy DS, Roy S, Casiano RR, Xue JW, Evans J. Acoustic analysis of the singing and speaking voice in singing students. J Voice. 2000;14(4):490–493. [CrossRef] [PubMed]
38. Sataloff RT. Care of the professional voice: use of instrumentation in the singing studio. J Sing. 2020;76(4):433–436.
39. Reetz S, Bohlender JE, Brockmann-Bauser M. Do standard instrumental acoustic, perceptual, and subjective voice outcomes indicate therapy success in patients with functional dysphonia? J Voice. 2019;33(3):317–324. [CrossRef] [PubMed]
40. Castelblanco L, Habib M, Stein DJ, de Quadros A, Cohen SM, Noordzij JP. Singing voice handicap and videostrobolaryngoscopy in healthy professional singers. J Voice. 2014;28(5):608–613. [CrossRef] [PubMed]
41. Kazi AA, Yu C, Vahidi NA, Donnell C, Moore JE. Longitudinal assessment of singing students. J Voice. 2023;37(1):145.e19–145.e21. [CrossRef] [PubMed]
42. Feinstein H, Daşdöğen Ü, Awan JA, Awan SN, Abbott KV. Comparative analysis of two methods of perceptual voice assessment. J Voice. 2025;39(4):1065–1075. [CrossRef] [PubMed]
43. Harris T, Howard D. The Voice Clinic Handbook. 2nd ed. Compton Publishing; 2018.
44. Iwarsson J. Effects of inhalatory abdominal wall movement on vertical laryngeal position during phonation. J Voice. 2001;15(3):384–394. [CrossRef] [PubMed]
45. Svec JG, Granqvist S. Guidelines for selecting microphones for human voice production research. Am J Speech Lang Pathol. 2010;19(4):356–368. [CrossRef] [PubMed]
46. Boersma P, Weenink D. Praat: doing phonetics by computer [Computer program]. Version 6.2.06, Copyright 1995–2025. 1992–2022. https://www.praat.org.
47. Lathadevi HT, Guggarigoudar SP. Objective acoustic analysis and comparison of normal and abnormal voices. J Clin Diagn Res. 2018;12(5):MC01–MC04. [CrossRef]
48. Yilmaz C, Bostancı Ö, Bulut S. Effect of respiratory muscle training on pitch range and sound duration in brass instrument players and singers. J Voice. 2022;36(1):76–82. [CrossRef] [PubMed]
49. Sobol M, Sielska-Badurek EM, Osuch-Wójcikiewicz E. Normative values for Singing Voice Handicap Index—systematic review and meta-analysis. Braz J Otorhinolaryngol. 2020;86(4):497–501. [CrossRef] [PubMed]
50. Lemon-McMahon B, Hughes D. Toward defining “vocal constriction”: practitioner perspectives. J Voice. 2018;32(1):70–78. [CrossRef] [PubMed]
51. Hixon TJ. Respiratory Function in Singers. Redington Brown; 2006.
52. Titze IR. Principles of Voice Production 2nd Printing. National Center for Voice and Speech; 2000.
Corresponding author: Ralph Magliano, School of Health Sciences, Harrisburg Area Community College, 1 HACC Drive, Harrisburg, PA 17110, USA. E-mail: Ralph.Magliano.Research@gmail.com Tel: +1-717-221-1386
COPYRIGHT
Published under the CreativeCommons Attribution-NonCommercial-NoDerivs 3.0 License.
International Journal of Therapeutic Massage and Bodywork, Volume 19, Number 2, June 2026