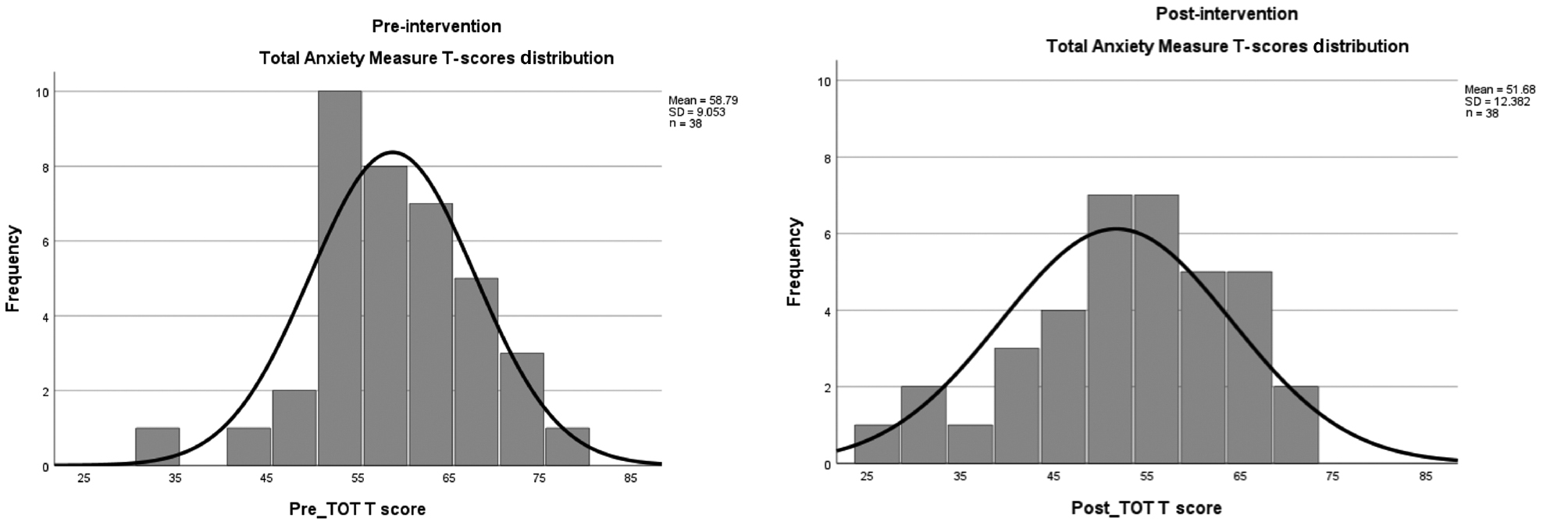
Figure 1. AMAS-C Total Anxiety T-scores (TOT) before and after massage therapy intervention, showing reduced anxiety following treatment. SD = standard deviation.
| International Journal of Therapeutic Massage and Bodywork (2026) 19(2), 14–26. | https://doi.org/10.3822/ijtmb.v19i2.1151 |
Jorge A. Pazmiño, PhD1*, Portia B. Resnick, PhD, ATC, BCTMB2
1W. Fielding Rubel School of Business, Bellarmine University, Louisville, KY, USA
2Department of Kinesiology, California State University Long Beach, Long Beach, CA, USA
Background: Anxiety is a prevalent concern among college students, impairing academic performance and increasing attrition risk for universities. Effective interventions are needed to reduce overall and test anxiety during high-stakes assessments.
Purpose: This study explored the effect of massage therapy (MT) in reducing overall and test anxiety in traditional-aged undergraduate business students compared to a comparison group engaged in a relaxation activity (adult coloring).
Setting: A private liberal arts university in the southeastern United States.
Participants: Undergraduate business students (aged 18–23 years) enrolled in accounting, business administration, finance, economics, or marketing.
Research Design: Quantitative, quasi-experimental, repeated-measures design with both within-subjects (pre–post) and between-subjects (MT vs. adult coloring) evaluations.
Intervention: The experimental group received a 30-min MT session administered by a licensed massage therapist 2 h prior to a final exam. The comparison group engaged in a 30-min adult coloring activity.
Main Outcome Measure: Anxiety levels were assessed pre- and post-intervention with the Adult Manifest Anxiety Scale—College Version (AMAS-C).
Results: MT significantly reduced overall anxiety (mean (M) = 58.79 to 51.68, t(37) = 4.103, p < 0.001, Cohen’s d = 0.666) and test anxiety (M = 59.29 to 55.24, t(37) = 2.623, p = 0.013, Cohen’s d = 0.426). Analyses of variance confirmed significant main effects of MT on overall anxiety (η2 = 0.314, p < 0.001) and test anxiety (η2 = 0.155, p = 0.015), unaffected by sex at birth or academic classification. Between-group differences with the comparison activity were not statistically significant (p = 0.114), though MT showed a small-to-moderate effect size.
Conclusion: A 30-min MT intervention effectively reduced overall and test anxiety among traditional-aged undergraduate business students when administered within a 2-h window prior to a final exam. MT demonstrates promise as a non-pharmacological strategy to support students during high-stakes academic assessments.
KEYWORDS: Overall anxiety; test anxiety; massage therapy; college students; higher education
While experiencing minor setbacks is beneficial for learning, it is essential to maintain a careful balance between gaining insights from these challenges and preventing a complete breakdown in academic progress.(1) Furthermore, due to society’s strong focus on upward progression and academic achievement, college students frequently grapple with a fear of failure, which can subsequently give rise to mental health challenges affecting their academic performance, specifically manifesting as anxiety.(2) Anxiety is characterized by the anticipation of a future real or perceived threat, resulting in sensations of tension, fear, and uneasiness.(3) While anxiety is a normal response to a stressful situation and occasional normal bouts can even be adaptive, helping individuals to stay alert and cautious, excessive or chronic anxiety can significantly impact the quality of life and well-being of an individual.(4) This state often coincides with heightened muscle tension and increased vigilance, as the nervous system responds to the possibility of perceived impending danger or other perceived negative events, potentially leading to cautious or avoidant behaviors.
The study by Li et al.,(5) which identified a significant association between anxiety symptoms and academic stress in college students, suggests that anxiety may hinder students’ ability to effectively process and respond to academic challenges, potentially impacting their academic success. Although undergraduate students prepare for a test or examination in advance, their efforts to perform well are hindered when they experience the pressure associated with failure. Often, anxiety acts as a memory blocker removing a student’s ability to recall answers from the knowledge acquired during a study session.(6) Moreover, Vitasari et al.(7) found that high levels of anxiety negatively impact students’ academic performance, as anxiety is a major predictor of lower examination scores and diminished study effectiveness.
In their research, Lipson et al.(8) identified anxiety as a widespread concern affecting most (73%) college students grappling with mental health issues (survey data from >350,000 students across 373 campuses). In addition, the American Psychological Association(9) asserts that test anxiety is a form of anxiety that arises from the pressure and uneasiness associated with assessment methods, often resulting in decreased performance. While not a formal diagnosis,(10) test anxiety is a well-documented psychological condition characterized by worry, nervousness, and fear before, during, or after assessments.(11,12) Physical symptoms commonly associated with test anxiety include sweating, trembling, nausea, increased heart rate, and even shortness of breath.(7) Experiencing test anxiety can lead to thoughts that can hinder a college student’s ability to focus, remember information, and perform well on assessments.(13) Since there is a lot at stake during their academic journey, for traditional-aged undergraduate business students completing courses such as accounting, finance, economics, marketing, or business administration, anxiety can negatively impact their academic performance. Without support, this effect can even influence their likelihood of staying in school, putting them at risk of dropping courses or potentially leaving college altogether.(14)
Additional factors that may influence anxiety levels include sex at birth and academic classification. Sex at birth has been explored in previous studies as a factor that may affect stress responses and coping mechanisms. Research indicates that males and females often exhibit varying physiological and psychological reactions to stress, potentially leading to different levels of responsiveness to anxiety-reducing interventions such as massage therapy (MT).(3,4) Including sex at birth as a variable allowed for a deeper understanding of whether MT has a universally positive impact or if its effectiveness varies by demographic factors. Similarly, academic classification was selected as a variable because lower-division (freshmen and sophomores) and upper-division (juniors and seniors) students typically experience different academic pressures and levels of familiarity with coping strategies. Research suggests that lower-division students, who are still adjusting to college demands, may experience higher levels of anxiety compared to upper-division students who have developed more refined coping skills.(3,5) Analyzing the MT intervention’s effectiveness across these classifications helps to identify whether specific academic stages influence outcomes.
According to the literature, suggestions for dealing with anxiety include using resources on campus, establishing a routine, approaching challenges with a positive outlook, resting, learning and implementing relaxation techniques, and developing a structured plan of action.(15–17) To improve their chances of success, it is essential for college students to adopt effective strategies for managing anxiety. Despite its potential to reduce anxiety, MT has not yet been recommended as a strategy for college student support. MT consists of the application of massage and non-hands-on components, including health promotion and education messages, for self-care and health maintenance.(18) Research studies affirm the efficacy of MT in alleviating anxiety and fostering relaxation by reducing stress hormones, such as cortisol.(19) However, the prevailing literature primarily stems from research conducted in healthcare settings, focusing on individuals experiencing various medical conditions and chronic pain.(20–22) This emphasizes an opportunity for further exploration of MT’s benefits in higher education, particularly in managing anxiety among different student demographics. Field et al.(19) reported that MT has a positive effect on anxiety. Yet, MT is currently underutilized by higher education institutions to intentionally support students in managing anxiety levels. In higher education, MT is mainly offered as a resource with the goal of promoting relaxation and well-being.(23) Although the literature offers ample evidence that MT can improve both physical and mental health,(20,22,24–31) its benefits are not intentionally utilized and measured in higher education to help students manage overall and test anxiety.
The study aimed to investigate the effects of MT compared to a comparison group on overall anxiety and test anxiety in traditional-aged undergraduate business students during the final exam period. Additionally, the study sought to examine the following:
The study employed a quantitative, quasi-experimental design to examine the effect of MT on anxiety levels in traditional-aged undergraduate business students at a private liberal arts university in the southeastern United States. A repeated-measures, between-subjects design was used, with participants assigned to either a 30-min MT session or a 30-min comparison activity (adult coloring book), both held 2 h before final exams. Anxiety levels were assessed pre- and post-intervention using the Adult Manifest Anxiety Scale—College Version (AMAS-C), enabling both within-subject and between-group comparisons.
The study received Institutional Review Board (IRB) approval (IRB#1123, December 1, 2023) under review (45 CFR 46, Category 7), ensuring compliance with ethical research standards. All participants provided informed consent digitally before data collection and received a written consent form to review prior to the intervention. Participation was voluntary, with the option to withdraw at any time. Data confidentiality was maintained through anonymized, securely stored responses. The research instrument remained unaltered, with copyright compliance ensured.
Participants were traditional-aged college students from 18 to 23 years old enrolled at a private liberal arts college in the southeastern United States pursuing an undergraduate degree in accounting, business administration, finance, economics, or marketing. The recruiting process of participants for the study happened through faculty notifications to students as well as targeted electronic communications to students advising them about the opportunity to participate. Furthermore, the study partnered with the institution’s Campus Recreation and Wellness Department to assist with awareness for participation. Students were not eligible if they were either outside of the age range or not enrolled in a business-related major. While the experimental group had strong engagement, participation in the comparison group was initially lower, likely due to the appeal of MT. To address this, the researcher actively recruited participants at a high-traffic location near the MT intervention site, leveraging direct engagement with potential participants and word of mouth.
The experimental group underwent a 30-min MT session, aimed at alleviating anxiety levels, which was scheduled 2 h before the participants’ final exams. The timing of the sessions was meticulously planned to accommodate the final exam schedule, with specific time slots allocated for interventions before exams at 8 am, 11:30 am, and 3 pm. This scheduling ensured that the MT occurred at an optimal time to potentially influence anxiety levels.
An experienced massage therapist, specializing in mental health, state-licensed, and insured, administered a 30-min massage session employing the following MT types/styles/techniques: Swedish massage, acupressure, cross-fiber friction, myofascial release, hydrotherapy, and aromatherapy. The MT practitioner adjusted the pressure applied based on the participant’s comfort level, using levels 1–3 on the Walton Pressure Scale. According to the Walton Pressure Scale, she employed either “light,” “medium,” or “heavy” pressure.(32)
The MT protocol used in the study was based on the Swedish massage technique, applied across various body areas in both supine and prone positions. The intervention was conducted in a dedicated, standard-sized study room (approximately 11 × 12 feet) within the business school’s common area, offering convenient access for the target population. While the room had windows facing the outdoors and the hallway, black cardboard panels were used to cover them, ensuring participant privacy and controlled lighting. All furniture was removed to create ample space for the massage table and the MT practitioner’s workspace. Fluorescent lighting was replaced with a table lamp to create a more conducive atmosphere. The room’s door could be secured from the inside with clear signage that the intervention was in progress. Table 1 provides a detailed overview of the specific techniques employed, including the targeted body areas, types of massage strokes, pressure levels according to the Walton Pressure Scale, and additional therapeutic elements incorporated to enhance the effectiveness of the treatment.
Table 1. Overview of Massage Therapy Techniques Used in the Session
| Body Area | Technique | Anatomical Focus | Pressure Level | Additional Notes |
|---|---|---|---|---|
| Supine position | ||||
| Shoulders | Bilateral effleurage/glides | Targeting upper and lower trapezius | Levels 1–3 (Walton Pressure Scale) | |
| Neck | Effleurage/glides, gentle acupressure | Focus on scalene muscles, suboccipital attachments | ||
| Scalp | Cross-fiber friction | Applied to temporalis muscles | Helps maintain soft tissue mobility and prevent adherent scar formation(33) | |
| Arms | Long broad strokes, petrissage | Includes forearm, bicep, deltoid | Levels 1–3 (Walton Pressure Scale) | Moderate pressure applied during petrissage |
| Hands | Spreading with compression, myofascial release | Focus on thenar and hypothenar eminences | Finished with hydrotherapy using hot towels | |
| Prone position | ||||
| Back | Bilateral effleurage/glides, myofascial release | Upper trapezius to crest of hip, paraspinal muscles | Levels 1–3 (Walton Pressure Scale) | Hydrotherapy with hot towels on the cervicothoracic region |
| Neck | Effleurage/glides, circular pressure | Focus on scalene muscles, suboccipital attachments | Peppermint essential oil applied | |
| Scalp | Cross-fiber friction | Applied with circular motion on temporalis muscles | ||
Each massage participant received a 30-min massage following the above protocol.
Participants allocated to the comparison group participated in a 30-min coloring session, an established anxiety-reduction activity reported in previous studies.(34) Once a design was selected from the book titled “Adult Coloring Book: Stress Relieving Designs Animals, Mandalas, Flowers, Paisley Patterns and So Much More,” participants received a pack of 24 pre-sharpened colored pencils manufactured by Crayola to engage in the coloring activity. All participants had the option to utilize a designated area in the student lounge to engage in this comparative relaxation method. They were informed that the duration of the coloring activity was limited to 30 min.
Demographic data including age, sex at birth, race, ethnicity, and academic classification were collected. Overall and test anxiety levels were measured two times during the experiment. Utilizing the AMAS-C survey, participants self-reported test anxiety levels as follows: (i) pre-intervention (experimental and comparison groups) and (ii) post-intervention (experimental and comparison groups). All responses were collected using Microsoft Forms. The AMAS-C survey instrument was sourced from the AMAS Manual.(35) The AMAS-C is a 42-item self-report instrument designed to assess manifest anxiety in college students across four subscales: Worry/Oversensitivity (12 items), Physiological Anxiety (8 items), Test Anxiety (15 items), and Social Concerns/Stress (7 items). The scale also includes a seven-item Lie scale to gauge response bias. Each item is answered with a simple “yes” or “no.” Within 2 h of an academic assessment, both groups self-reported their anxiety levels (pre-intervention score). The experimental group then received MT while the comparison group participated in a coloring activity. Immediately afterward and prior to an academic assessment, both groups self-reported their anxiety levels again (post-intervention score).
Data collection was managed through Microsoft Forms by creating pre- and post-intervention forms for each group. To ensure accessibility, four unique QR codes linked participants to their respective forms. Pre-intervention QR codes were distributed at the intervention site, granting mobile access to the survey and a digital consent form. The identities of all participants were kept confidential, and the massage therapist did not collect any data.
For scoring, the AMAS-C provides an Overall Anxiety measure by summing all the items from the subscales, with a maximum score of 42. To obtain the test anxiety score, the 15 Test Anxiety items were totaled. The instrument uses T-scores to interpret results, offering five categories: extreme, clinically significant, slight elevation, expected, and low anxiety, each with specific implications for anxiety levels. Lowe developed T-scores based on a sample of 818 traditional college students.(33) Lowe’s research provides robust normative data to support the interpretation of anxiety levels, with specific attention to the Test Anxiety subscale, for identifying students at risk of performance impairment due to anxiety. Throughout the manuscript, the term T-scores will be used to represent the converted scores of the AMAS-C for all participants in the study.
Data were imported from Microsoft Forms into an Excel file. Subsequently, all responses were coded in numerical form to reflect four AMAS-C subscales that were identified by each survey item. Then, all raw scores were converted to T-scores utilizing the AMAS-C conversion tables as described above and were analyzed using the Statistical Package for the Social Sciences, Version 29.0 (SPSS, IBM, Armonk, NY, USA). Descriptive statistics were employed to summarize demographic data for both the experimental and comparison groups separately.
To compare the pre- and post-intervention survey scores, a paired t-test was used. An independent samples t-test was employed to observe any differences between the effect of the intervention (MT) versus the comparison activity (adult coloring book) post-intervention. To identify variations in the effect of MT based on sex at birth and academic classification, several two-way mixed analyses of variance (ANOVAs) were conducted. The independent variables were overall anxiety score and the Test Anxiety subscale score as described by the AMAS-C conversion table. The dependent variables were sex at birth, either male or female, and academic classification, either lower division (freshman or sophomore) or upper division (junior or senior).
The experimental group consisted of 38 traditional-aged undergraduate business students. Table 2 presents summary descriptive data using “male” and “female” as the two classifications for the experimental group’s sex at birth. Additional information to illustrate characteristics for the experimental group covered age, race/ethnicity, academic classification, and academic major.
Table 2. Participant Demographics and Academic Characteristics
| Characteristic | Category | Experimental Group, n (%) | Comparison Group, n (%) |
|---|---|---|---|
| Sex at birth | Male | 19 (50.0) | 16 (42.1) |
| Female | 19 (50.0) | 22 (57.9) | |
| Age (years) | 18 | 7 (18.4) | 3 (7.9) |
| 19 | 12 (31.6) | 9 (23.7) | |
| 20 | 9 (23.7) | 11 (28.9) | |
| 21 | 7 (18.4) | 7 (18.4) | |
| 22 | 1 (2.6) | 4 (10.5) | |
| 23 | 2 (5.3) | 4 (10.5) | |
| Race/ethnicity | African American/Black | 4 (10.5) | 5 (13.2) |
| Asian | 2 (5.3) | 4 (10.5) | |
| Hispanic/Latino(a) | 5 (13.2) | 6 (15.8) | |
| White | 26 (68.4) | 22 (57.9) | |
| Other | 1 (2.6) | 1 (2.6) | |
| Academic classification | Lower division | 20 (52.6) | 12 (31.6) |
| Upper division | 18 (47.4) | 26 (68.4) | |
| Major/minor | Accounting | 3 (7.9) | 5 (13.2) |
| Business Administration | 23 (60.5) | 25 (65.8) | |
| Economics | 2 (5.3) | 1 (2.6) | |
| Finance | 6 (15.8) | 4 (10.5) | |
| Marketing | 4 (10.5) | 3 (7.9) |
The comparison group consisted of 38 traditional-aged undergraduate business students. Table 2 presents summary descriptive data using “male” and “female” as the two classifications for the comparison group’s sex at birth. Additional information to illustrate characteristics for the comparison group covered age, race/ethnicity, academic classification, and academic major.
The Shapiro–Wilk test confirmed normal distribution of pre- and post-intervention anxiety scores (p > 0.05). Levene’s test was used to assess the homogeneity of variances prior to conducting ANOVA. It was applied to anxiety scores across the experimental and comparison groups (F = 2.331, p = 0.131), sex at birth (F = 0.946, p = 0.334), and academic classification (F = 5.625, p = 0.022). Therefore, the use of parametric analyses was validated.(36)
A paired samples t-test revealed that overall anxiety scores, as measured by the AMAS-C and shown in Figure 1, were significantly lower post-intervention (mean (M) = 51.68, standard deviation (SD) = 12.38) compared to pre-intervention (M = 58.79, SD = 9.053, t(37) = 4.103, p < 0.001, d = 0.666) (Table 3). MT showed statistical significance in reducing overall anxiety levels among traditional-aged undergraduate business students, with scores decreasing following the intervention. This reduction, ranging from 3.6 to 10.6 points, was supported by a moderate to large effect size (Cohen’s d = 0.666) and a moderate positive correlation between pre- and post-intervention scores (r = 0.541, p < 0.001).
Figure 1. AMAS-C Total Anxiety T-scores (TOT) before and after massage therapy intervention, showing reduced anxiety following treatment. SD = standard deviation.
Table 3. Experimental Group: Pre- and Post-Intervention Anxiety Scores
| Measure | Pre Mean (SD) | Post Mean (SD) | Mean Difference (95% CI) | t (df) | p-value/Effect Size |
|---|---|---|---|---|---|
| Overall anxiety | 58.79 (9.05) | 51.68 (12.38) | 7.11 (3.60–10.61) | t = 4.10 (37) | p < 0.001, d = 0.67 (0.31–1.01) |
| Test anxiety | 59.29 (10.13) | 55.24 (12.08) | 4.05 (0.92–7.18) | t = 2.62 (37) | p = 0.013, d = 0.43 (0.09–0.76) |
CI = confidence interval; SD = standard deviation.
A paired samples t-test showed that test anxiety scores were significantly lower post-intervention (M = 55.24, SD = 12.082) compared to pre-intervention (M = 59.29, SD = 10.126, t(37) = 2.623, p = 0.013, d = 0.426) (Table 3). MT reduced test anxiety levels among traditional-aged undergraduate business students. There was a moderate effect size (Cohen’s d = 0.426) and a strong positive correlation between pre- and post-intervention scores (r = 0.645, p < 0.001).
An independent samples t-test indicated that while the MT intervention group had a lower overall anxiety score following the intervention (M = 51.68, SD = 12.382) compared to the comparison group (M = 56.58, SD = 14.229), the change was not statistically significant, t(74) = −1.60, p = 0.114, d = 0.37. While Cohen’s d indicated a small to medium effect size, the effects were not statistically significant (Table 4).
Table 4. Comparison Group Results
| Measure | Pre Mean (SD) | Post Mean (SD) | t (df) | p-value | 95% CI |
|---|---|---|---|---|---|
| Total anxiety (comparison group) | 60.03 (13.08) | 56.58 (14.23) | t = −1.60 (74) | p = 0.057 | −10.99 to 1.20 |
CI = confidence interval; SD = standard deviation.
A two-way mixed ANOVA was conducted to examine the effects of sex at birth and the MT intervention on the Overall Anxiety Measure T-scores (Table 5). The results of the ANOVA revealed that the MT intervention exhibited a significant main effect on Overall Anxiety Measure T-scores, f(1, 36) = 16.452, p < 0.001, η2 = 0.314, with a large effect size (0.314).(37) However, sex at birth had a significant influence on Overall Anxiety Measure T-scores, f(1, 36) = 3.925, p = 0.055, η2 = 0.098. Additionally, there was no significant interaction between sex at birth and the MT intervention, f(1, 36) = 0.153, p = 0.698, η2 = 0.004.
Table 5. Within-Subjects Effects (Repeated-Measures ANOVA)
| Source | SS | df | MS | F | p/η2 |
|---|---|---|---|---|---|
| Overall anxiety × sex at birth | 959.21 | 1 | 959.21 | 16.45 | p < 0.001, η2 = 0.314 |
| Test anxiety × sex at birth | 312.05 | 1 | 312.05 | 6.71 | p = 0.014, η2 = 0.157 |
| Overall anxiety × academic classification | 928.42 | 1 | 928.42 | 16.45 | p < 0.001, η2 = 0.314 |
ANOVA = analysis of variance; MS = mean square; SS = sum of squares; η2 = eta squared (effect size).
A two-way mixed ANOVA was conducted to examine the effects of sex at birth and the MT intervention on the Test Anxiety Subscale T-scores (Table 5). The results of the ANOVA exposed a significant main effect of MT intervention on Test Anxiety Subscale T-scores, f(1, 36) = 6.708, p = 0.014, η2 = 0.157, with a large effect size (0.157).(37) However, the interaction effect between Test Anxiety Subscale T-scores and sex at birth did not attain statistical significance, f(1, 36) = 0.072, p = 0.789, η2 = 0.002.
A two-way mixed ANOVA was conducted to examine the effects of academic classification (upper division vs. lower division) and the MT intervention on the Total Anxiety Measure T-scores (Table 5). The results of the ANOVA revealed a significant main effect of the MT intervention on Total Anxiety Measure T-scores, f(1, 36) = 16.448, p < 0.001, η2 = 0.314, with a large effect size (0.314).(37) However, academic classification did not significantly influence the Total Anxiety Measure T-scores, f(1, 36) = 2.235, p = 0.144, η2 = 0.058. Moreover, the interaction between the MT intervention and academic classification did not reach statistical significance, f(1, 36) = 1.343, p = 0.254, η2 = 0.036.
A two-way mixed ANOVA was conducted to examine the effects of academic classification and the MT intervention on the Test Anxiety Subscale T-scores (Table 6). The results of the ANOVA revealed a statistically significant main effect of the MT intervention on test anxiety levels, f(1, 36) = 6.582, p = 0.015, η2 = 0.155, with a large effect size (0.155).(37) In addition, there was a significant effect of academic classification on Test Anxiety Subscale T-score, f(1, 36) = 3.940, p = 0.055, η2 = 0.099. Moreover, the interaction effect between the MT intervention and academic classification was not statistically significant, f(1, 36) = 0.841, p = 0.365, η2 = 0.023.
Table 6. Between-Subjects Effects (Test Anxiety × Academic Classification)
| Source | SS | df | MS | F | p/η2 |
|---|---|---|---|---|---|
| Intercept | 249,949.87 | 1 | 249,949.87 | 1,328.09 | p < 0.001, η2 = 0.974 |
| Academic classification | 741.45 | 1 | 741.45 | 3.94 | p = 0.055, η2 = 0.099 |
| Error | 6,775.29 | 36 | 188.20 |
MS = mean square; SS = sum of squares; η2 = eta squared (effect size).
The MT intervention demonstrated a significant reduction in anxiety levels among traditional-aged undergraduate business students. Participants experienced a noticeable decrease in their overall anxiety after the intervention, which suggests that MT can be an effective method for promoting relaxation during high-pressure academic periods like finals week. The study also focused specifically on test anxiety, finding that MT had a meaningful impact on lowering test anxiety in this sample. There is an indication of potential benefit to offering MT as a supportive strategy for students struggling with anxiety stemming from traditional assessments embedded within higher education. While MT significantly reduced overall and test anxiety in traditional-aged undergraduate business students during high-stakes assessment periods such as finals week, the comparison group of an adult coloring book activity did not show a significant change in overall or test anxiety.
To compare its effectiveness against another established anxiety-reduction technique,(34) adult coloring was used as an active comparator to assess the effect of MT on overall and test anxiety. Research has consistently shown that MT effectively reduces anxiety and stress due to its ability to lower cortisol levels and promote parasympathetic nervous system activity.(19) The findings of the study revealed that the coloring book has a smaller impact on the responses associated with overall and test anxiety within the same treatment window as MT as assessed by the AMAS-C, based on the variability in responses observed within the comparison group. Adding to existing literature suggesting that MT has the potential to reduce anxiety,(19,25,26) the results of the current research study demonstrate MT’s effectiveness in addressing anxiety when compared to adult coloring, reaffirming the potential MT can have in anxiety management protocols.
In addition, it was hypothesized that MT would affect participants differently based on sex at birth and academic classification. Female participants were expected to be more receptive to anxiety-reduction strategies(38,39); however, the findings showed no significant differences between males and females in terms of anxiety reduction. Both groups benefited equally from the MT intervention. Likewise, it was initially expected that lower-division students (freshmen or sophomores) would respond more favorably to the MT intervention than upper-division students (juniors and seniors). This expectation was based on the literature suggesting that lower-division students tend to be more adaptable,(40) face less academic pressure,(41) and are more open to trying new anxiety management strategies.(42) Nevertheless, the study found that the reduction in anxiety was consistent across both groups, regardless of academic classification. One possible explanation for this consistent effect could be the timing and structure of the MT intervention. The intervention took place at the end of the fall semester, coinciding with the first time lower-division students, specifically freshmen, faced final examinations in college. Additionally, the intervention was implemented over a condensed 5-day period. Following a precise protocol of 30-min sessions scheduled 2 h before the participants’ final exams, the experiment ensured that the MT was administered at an optimal time to potentially influence anxiety levels. The carefully coordinated schedule likely maximized the potential impact of the MT on overall and test anxiety, explaining the consistent results across groups.
Overall, the findings of the study highlight MT as a promising tool for reducing both overall and test anxiety among traditional-aged undergraduate business students during finals week, regardless of sex at birth or academic classification. Given these findings, colleges and universities might consider incorporating MT into their student support services to help manage anxiety leading to assessment periods such as finals week.
There are several limitations that may have introduced confounding variables and affected generalizability. The quasi-experimental design, with participants self-selecting into the MT or adult coloring book group, introduced selection bias. While randomization was considered, time constraints prevented its implementation, further limiting internal validity. Recruitment challenges, likely due to the less appealing nature of the comparison activity, also influenced the study. Efforts to balance group sizes may have unintentionally altered the characteristics of the comparison group, introducing bias. The small sample size (n = 38) limits statistical power and generalizability. However, converting the AMAS-C scores to standardized scores as described in the literature helped mitigate this limitation.(33) Finally, while a consistent protocol was followed, using a single licensed massage therapist may affect replicability, as variations in therapeutic approach could influence intervention execution.
The study provides valuable insights but highlights areas for further exploration. Future studies could examine MT across disciplines such as education, health sciences, liberal arts, and STEM to identify discipline-specific stressors and tailor interventions. Qualitative research could deepen understanding of students’ emotional, cognitive, and social experiences with MT, while longitudinal studies tracking MT from freshman to senior year could assess long-term effectiveness. Also, expanding research to graduate students, who face unique academic pressures, would enhance applicability. Further longitudinal studies are needed to evaluate MT’s sustained impact on anxiety and academic outcomes like GPA or retention, determining optimal session frequency and duration. Lastly, assessing the feasibility of integrating MT into educational settings, considering logistical challenges, costs, and barriers like stigma or awareness, could help institutions implement evidence-based student support strategies.
A 30-min MT intervention effectively reduced overall and test anxiety among traditional-aged undergraduate business students when administered within a 2-h window prior to a final exam. Moderate to large effect sizes indicate that the MT intervention made a meaningful difference in lowering anxiety levels. As measured by the AMAS-C, the reduction in overall and test anxiety in the MT group was statistically significant and uninfluenced by sex at birth or academic classification. Although the MT group exhibited lower post-intervention anxiety levels compared to the compassion group, the between-group difference was not statistically significant. Nonetheless, both groups experienced anxiety reductions, suggesting that each intervention served its intended purpose. The consistent and statistically significant reduction in anxiety within the MT group highlights its effectiveness as a strategy for alleviating anxiety during high-stakes academic assessments.
The massage therapist who developed and administered the intervention is the spouse of the primary investigator. This relationship has been disclosed. The therapist was not involved in data analysis or outcome assessment, and steps were taken to minimize potential bias.
No sources of funding were used in this study.
Jorge A. Pazmiño was responsible for study conception and design, data analysis, and manuscript preparation. The massage therapy protocol used in this study was developed and administered by a licensed massage therapist (Lauren Pazmiño, LMT), who delivered the intervention to participants. Portia B. Resnick served as a subject matter expert, offering professional perspective on the massage therapy protocol and providing guidance on study design and the use of a comparison group. She also contributed to manuscript writing, editing, and mentorship.
1. Choi B. I’m afraid of not succeeding in learning: introducing an instrument to measure higher education students’ fear of failure in learning. Stud High Educ. 2021;46(11):2107–2121. [CrossRef]
2. O’Donnell PS. Executive functioning profiles and test anxiety in college students. J Psychoeduc Assess. 2017;35(5):447–459. [CrossRef]
3. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013. [CrossRef]
4. Penninx BW, Pine DS, Holmes EA, Reif A. Anxiety disorders. Lancet. 2021;397(10277):914–927. [CrossRef] [PubMed]
5. Li W, Zhao Z, Chen D, Peng Y, Lu Z. Prevalence and associated factors of depression and anxiety symptoms among college students: a systematic review and meta-analysis. J Child Psychol Psychiatry. 2022;63(11):1222–1230. [CrossRef] [PubMed]
6. Kenya A, Vuyiya C. The neurobiological effect of anxiety and depression on memory in academic learning: a literature review. J Contemp Chiropr. 2020;3:36–44.
7. Vitasari P, Wahab MNA, Othman A, Herawan T, Sinnadurai SK. The relationship between study anxiety and academic performance among engineering students. Procedia Soc Behav Sci. 2010;8:490–497. [CrossRef]
8. Lipson SK, Zhou S, Abelson S, Heinze J, Jirsa M, Morigney J, et al. Trends in college student mental health and help-seeking by race/ethnicity: findings from the national healthy minds study, 2013–2021. J Affect Disord. 2022;306:138–147. [CrossRef] [PubMed]
9. American Psychological Association. APA Dictionary of Psychology. 2023. Available from: https://dictionary.apa.org/. Accessed July 6, 2023.
10. Putwain DW, Stockinger K, von der Embse NP, Suldo SM, Daumiller M. Test anxiety, anxiety disorders, and school-related wellbeing: manifestations of the same or different constructs? J Sch Psychol. 2021;88:47–67. [CrossRef] [PubMed]
11. Grant AD. An ESL instructor’s guidebook for reducing test anxiety at the community college level through exploring alternatives in assessment. Master’s Projects and Capstones. University of San Francisco, 2016. Available from: https://repository.usfca.edu/capstone/461. Published December 16, 2016.
12. Sucuoğlu E. Analysis of overseas students’ level of test anxiety according to their demographic characteristics. Qual Quant. 2018;52(Suppl 1):389–396. [CrossRef]
13. Enright M, Baldo TD, Wykes SD. The efficacy of eye movement desensitization and reprocessing therapy technique in the treatment of test anxiety of college students. J Coll Counsel. 2000;3(1):36–48. [CrossRef]
14. Kuh GD, Kinzie JL, Buckley JA, Bridges BK, Hayek JC. What Matters to Student Success: A Review of the Literature. Vol. 8. National Postsecondary Education Cooperative; 2006.
15. Hembree R. Correlates, causes, effects, and treatment of test anxiety. Rev Educ Res. 1988;58(1):47–77. [CrossRef]
16. Morton DP, Hinze J, Craig B, Herman W, Kent L, Beamish P, et al. A multimodal intervention for improving the mental health and emotional well-being of college students. Am J Lifestyle Med. 2020;14(2):216–224. [CrossRef] [PubMed]
17. Zeidner M. Test Anxiety: The State of the Art. Kluwer Academic Publishers; 1998. [CrossRef]
18. Kennedy AB, Cambron JA, Sharpe PA, Travillian RS, Saunders RP. Clarifying definitions for the massage therapy profession: the results of the best practices symposium. Int J Ther Massage Bodywork. 2016;9(3):15–26. [CrossRef] [PubMed]
19. Field T, Hernandez-Reif M, Diego M, Schanberg S, Kuhn C. Cortisol decreases and serotonin and dopamine increase following massage therapy. Int J Neurosci. 2005;115(10):1397–1413. [CrossRef] [PubMed]
20. Hall H, Munk N, Carr B, Fogarty S, Cant R, Holton S, et al. Maternal mental health and partner-delivered massage: a pilot study. Women Birth. 2021;34(3):e237–e247. [CrossRef] [PubMed]
21. Munk N, Harrison A. Integrating the international classification of functioning, disability, and health model into massage therapy research, education, and practice. Int J Ther Massage Bodywork. 2010;3(4):29–36. [CrossRef] [PubMed]
22. Munk N, Kruger T, Zanjani F. Massage therapy usage and reported health in older adults experiencing persistent pain. J Altern Complement Med. 2011;17(7):609–616. [CrossRef] [PubMed]
23. McElligott D, Siemers S, Thomas L, Kohn N. Health promotion in nurses: is there a healthy nurse in the house? Appl Nurs Res. 2009;22(3):211–215. [CrossRef] [PubMed]
24. Li Z, Bauer B, Aaberg M, Pool S, Van Rooy K, Schroeder D, et al. Benefits of hand massage on anxiety in preoperative outpatient: a quasi-experimental study with pre- and post-tests. Explore (NY). 2021;17(5):410–416. [CrossRef] [PubMed]
25. Meier M, Unternaehrer E, Dimitroff SJ, Benz ABE, Bentele UU, Schorpp SM, et al. Standardized massage interventions as protocols for the induction of psychophysiological relaxation in the laboratory: a block randomized, controlled trial. Sci Rep. 2020;10(1):14774. [CrossRef] [PubMed]
26. Moyer CA, Rounds J, Hannum JW. A meta-analysis of massage therapy research. Psychol Bull. 2004;130(1):3–18. [CrossRef] [PubMed]
27. Edge J. A pilot study addressing the effect of aromatherapy massage on mood, anxiety and relaxation in adult mental health. Complement Ther Nurs Midwifery. 2003;9(2):90–97. [CrossRef] [PubMed]
28. Mamtani R, Cimino A. A primer of complementary and alternative medicine and its relevance in the treatment of mental health problems. Psychiatr Q. 2002;73(4):367–381. [CrossRef] [PubMed]
29. Noto Y, Kudo M, Hirota K. Back massage therapy promotes psychological relaxation and an increase in salivary chromogranin a release. J Anesth. 2010;24(6):955–958. [CrossRef] [PubMed]
30. Post-White J, Fitzgerald M, Savik K, Hooke MC, Hannahan AB, Sencer SF. Massage therapy for children with cancer. J Pediatr Oncol Nurs. 2009;26(1):16–28. [CrossRef] [PubMed]
31. Rapaport MH, Schettler PJ, Larson ER, Edwards SA, Dunlop BW, Rakofsky JJ, et al. A preliminary descriptive report of the longevity of the effects of Swedish massage therapy for subjects with generalized anxiety disorder. J Bodyw Mov Ther. 2023;33:176–181. [CrossRef] [PubMed]
32. Walton T. Medical Conditions and Massage Therapy: A Decision Tree Approach. Jones & Bartlett Learning; 2020.
33. Lowe PA. Validation of the Adult Manifest Anxiety Scale–College Version scores in a sample of U.S. college students. Can J Sch Psychol. 2013;28(3):277–294. [CrossRef]
34. Flett JAM, Lie C, Riordan BC, Thompson LM, Conner TS, Hayne H. Sharpen your pencils: preliminary evidence that adult coloring reduces depressive symptoms and anxiety. Creativity Research Journal. 2017;29(4):409–416. [CrossRef]
35. Reynolds CR, Richmond BO, Lowe PA. The Adult Manifest Anxiety Scale (AMAS): Manual. Western Psychological Services (WPS); 2003. Available from: https://books.google.com/books?id=9KdUlQEACAAJ
36. Field, A. Discovering Statistics Using IBM SPSS Statistics. 5th ed. SAGE Publications; 2023.
37. Cohen, J. A power primer. Psychol Bull. 1992;112(1):155–159. [CrossRef] [PubMed]
38. Graves BS, Hall ME, Dias-Karch C, Haischer MH, Apter C. Gender differences in perceived stress and coping among college students. PLoS One. 2021;16(8):e0255634. [CrossRef] [PubMed]
39. Rausch SM, Auerbach SM, Gramling SE. Gender and ethnic differences in stress reduction, reactivity, and recovery. Sex Roles. 2008;59(9–10):726–737. [CrossRef]
40. Tinto V. Leaving College: Rethinking the Causes and Cures of Student Attrition. University of Chicago Press; 1993. Available from: https://books.google.com/books?id=AB-ERLYDMg8C
41. Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469–480. [CrossRef] [PubMed]
42. Conley CS, Shapiro JB, Huguenel BM, Kirsch AC. Navigating the college years: developmental trajectories and gender differences in psychological functioning, cognitive-affective strategies, and social well-being. Emerg Adulthood. 2020;8(2):103–117. [CrossRef]
Corresponding author: Jorge A. Pazmiño, PhD, W. Fielding Rubel School of Business, Bellarmine University, 2001 Newburg Rd, Louisville, KY 40205, USA. E-mail: jpazmino@bellarmine.edu Tel: +1-502-272-7240
COPYRIGHT
Published under the CreativeCommonsAttribution-NonCommercial-NoDerivs3.0License.
International Journal of Therapeutic Massage and Bodywork, Volume 19, Number 2, June 2026